May each of you be Blessed with a Healthy New Year. The APF will continue to be available to you and your families. We will be implementing and help facilitate exciting new projects in the coming year to include:
~ Print Five new brochures ~ Family education project ~ Expand and update APF website ~ Post Knowledgeable doctors on the APF website ~ Facilitate Eight research projects ~ Host a Series of Patient support meetings around the county (first meeting is January 31, 2014)
~ Expand porphyria clinics around the country ~ Enlarge Protect the Future program to train future experts ~ Host physicians on our five Facebook groups ~ Host primary care physician training program ~ And much, much more
Watch for news of each additional project starting with details on our first patient education meeting.
"Remember..Research is the key to your cure!"
Happy 2014!
New exciting Information on Porphyria & how you can help!
Friday - December 27, 2013 @ 15:36:34
Join the Registry
Join the Porphyria Registry and LET THE GOVERNMENT KNOW THEY MUST PROVIDE FUNDING FOR PORPHYRIA RESEARCH!!!!!
To join the Contact Registry, click here to open a page that lists all of the rare disease consortia. Scroll down the page until you come to the Porphyria Consortium and click on your type of porphyria. You will then be asked to complete a simple form including information about the date of your diagnosis, if you know it. If you have copies of your initial diagnostic lab results, you may want to have them handy when you go to the registry website.
Porphyria experts have created this National Porphyria Registrya type of partnership between doctors and patients as a way for those with porphyria to share information about their health and treatment so physicians can learn from their experience and use that knowledge to enhance diagnosis, treatment and eventually find a cure for porphyria.
It is the best means to prove that there are enough porphyria patients who want improved health care. If we don't speak up, we will be left behind when research funding is given. We DO NOT HAVE ENOUGH PEOPLE ON THE REGISTRY. Please join the registry.
Joining the Porphyria Registry is anonymous and free of charge. All data will be stored in a secure, computerized database. No personal identifying information (such as your name, address, telephone number) will be given to anyone without your expressed approval.
Doctors who study rare diseases see a relatively small number of sufferers over many years of practice. This Registry will give a big boost to medical and scientific understanding of porphyria by bringing together information from patients all over the country.
If you need help enrolling in the registry contact our office toll free at
1-866-APF-3635
"Remember..Research is the key to your cure!"
Liver Foundation Facts
Wednesday - December 25, 2013 @ 10:00:03
This is from the Liver Foundation Fact: Liver Fact: The liver is a storage site for a variety of substances. It houses supplies of glycogen as well as numerous vitamins like A, D, K, and B12- to be used months and sometimes years later!
LIVER FACTS
The liver is the largest solid organ in our body. Its about 8 inches (20 cm) wide, 6.5 inches (17 cm) long and 4.5 inches (12 cm) thick and weighs approximately 3.5 pounds (1.6 kilograms).
Youll find your liver mostly under your ribs in the upper right part of your abdomen, just below your diaphragm.
The liver has two large lobes; a large right lobe and a smaller left lobe.
The liver has various functions:
It makes and secretes bile to help your body absorb fats and fat-soluble vitamins (A, D, E and K)
It metabolizes and stores carbohydrates, fats, sugars, vitamins (and other nutrients obtained from the foods we eat) for energy and brain function.
It breaks down harmful chemicals (bilirubin and ammonia) produced by the body and keeps the body regulated and healthy.
It manufactures proteins to help maintain blood purity and proper flow.
It breaks down hormones, detoxifies water and removes drugs, alcohol and environmental toxins
And it filters waste products from your blood.
Trouble is; the liver also stores all the toxins that our body cannot break down.
You see the liver is broken into three zones, each with a specific function. The blood enters the first zone, travels to the second and third zone then leaves the liver - with each zone being susceptible to its own illnesses.
Amazingly, the liver can regenerating itself, however today with the consistent abuse from our fast paced lifestyle our liver is paying a hefty price.
Dangerous Eating Habits
Studies show that a fast food diet of burgers, fries and soft drinks can damage the liver.
It is normal for your liver to contain some fat, but if the weight of your liver is more than 10% fat, then you have fatty liver and you may develop more serious complications.
When we eat too much fatty food it increases an enzyme called alanine aminotransferase (ALT) an enzyme which indicates liver damage and increases the risk of developing Type 2 diabetes, as well as hepatitis C.
Fat cells are building up in the liver and endangering our health. Due to our modern lifestyles, doctors are seeing a wide range of preventable illnesses.
The deficiencies in our diet as well as the excessive and habitual consumption of alcohol, tobacco, caffeine, food additives, pharmaceutical and OTC (over-the-counter) drugs are killing our liver cells.
Plus, environmental pollutants such as garden chemicals, cosmetic ingredients, home repair materials and household cleaning products are overtaxing our liver.
A damaged liver has difficulty removing toxins. And, if toxins remain in our system they can build up in our blood and our brain.
A struggling liver can cause a variety of health problems, including:
Headaches
Dark urine
Loss of appetite
Nausea and vomiting
Diarrhea, and light colored stools
Enlarged blood vessels, easy bruising
Anxiety and depression
Mental confusion
PMS
Exhaustion and fatigue
Jaundice, or yellowing of the skin
Impaired libido (sex drive)
Food allergies and chemical sensitivities
"Remember..Research is the key to your cure!"
Happy & Healthy New Year to You!
Monday - December 23, 2013 @ 10:43:42
Merry Christmas, Happy Holidays, Happy, Healthy New Year!
May you be blessed with happiness, good health, love and the delight of being with family and friends this wonderful Christmas and Holiday Season.
The opportunity to serve you and your family during this past year has been a gratifying experience for us.
Our staff and support volunteers look forward to meeting and assisting you throughout the upcoming Year.
We wish You All a Happy, Healthy New Year!
God Bless YOU!
Yvette, Elizabeth, Susan, Carol, Warren, Desiree and Facebook Team: Rob, Amy C, Amy B, Victor, Ben, Pierre
Wishing you warm holiday greetings from the team at RareConnect
Thanks for being a member of RareConnect.org
Connecting Rare Disease Patients Globally
"Remember..Research is the key to your cure!"
A Story from Jennifer Wood and her journey with EPP
Thursday - December 19, 2013 @ 22:00:06
Jennifer Wood
Type of Porphyria:
Erythropoietic Protoporphyria (EPP)
All my life I have been an indoor kind of girl. I really didn't think I had much of a choice. Every time I went outside, I was in excrutiating pain. Before I was even old enough to know better, I would stay indoors.
When I was about 18 months old, my mom took me to the beach near where we lived in Florida. Within a half hour, I started screaming. Nothing could be physically seen wrong with me until the swelling started. Then I turned purple, so when the doctors saw me, they said I had been stung by a jelly fish. It seemed logical to my parents. Months later the same thing happened and the doctors said it must have been caused by decomposed jelly fish, or maybe even an allergic reaction to the sunscreen. Each time it ended the same; me swollen and purple and the doctors not knowing the cause.
As I got older, I learned to adapt by wearing certain clothing and staying out of the sun. If I was forced to go outside for some reason or another, I was very quick to spot the shaded areas so the pain could be lessened a bit. My clothing tends to look a bit extravagant, especially my Sunday dress. When I take a simple dress; add long satin gloves, big hats (always nicely decorated to match dress) and topped off with a parasol, people just think I'm an extravagant person. It's easier for me if they think that than have to explain to them that sunlight is painful.
At work my co-workers call me the "vampire" because I work in a dark corner with all my windows covered. Any time I have to walk outside, I have on a big hat and gloves. For me my biggest frustration is that I only got my diagnosis in October 2005. I am a 28 year old woman who was thought to be crazy by everyone elseeven doctorsuntil the diagnosis. I have been told that it was only in my head and that the sun could not be hurting me until my last episode.
Last June, I was outside staying in the shade the entire time and again it was for only about 30 mintues. Even with my long sleeved shirt, my arms were stinging, my hands swelled up, my eyes swelled shut and every part of me that wasn't covered with heavy fabric turned purple. I spent a couple days crying in pain. One night during this period, I couldn't sleep so I got up and decided to watch a movie. It was about children who couldn't be exposed to sunlight. I watched the extra features and found there are a number of diseases that made sunlight painful. So I went on-line, researched them, and found the APF. They lead me to a dermatologist. I went to the only local dermatologist in my area. He then sent me to Vanderbilt because he admitted that my case was a bit out of his range.
That doctor was wonderful. She talked to me, asking questions I never thought were relevant, like what happend when my gall-bladder was removed. And after a good long while, she looked up at me said, "We'll have to do some tests to make sure, but I bet the farm it's porphyria." Then after all the blood tests came back, she knew she was right. I had EPP. If I could have hugged her through the phone, I would have. To finally have a name for what's wrong with me, know that there are others out there like meand know that I'm not crazywas a real relief.
Since my diagnosis, I have been involved in seminars at Vanderbilt about rare skin conditions and diseases. They also want me for the liver seminars in the future. I gladly volunteer to help spread some light on this disease that so many doctors know nothing about, so maybe someone else in the future can have a quicker recognition of their condition than what I had.
"Remember..Research is the key to your cure!"
AIP: An Educational Webcast For ED Providers
Wednesday - December 18, 2013 @ 20:14:19
In this webcast, Eric Gross, MD, describes the gastrointestinal, neurological, cardiovascular, and urologic symptoms of AIP. He explains the precipitating factors that may lead to an AIP attack and also outlines the diagnostic pathway and the commonly used tests to screen for AIP.
Dr. Gross is a faculty physician in the Department of Emergency Medicine at Hennepin County Medical Center, Minneapolis, Minnesota. He is also a professor of emergency medicine at the University of Minnesota Medical School.
Were so glad to have you here. Who ever signs up to the Purple Light Blog and is the 100th person will receive a gift from the APF. So what are you waiting for who's going to win?
Suffer from Chronic Pain watch this EMC course on Discovery Channel
Saturday - December 14, 2013 @ 10:30:01
100 million American adults live with chronic pain. That's more than cancer, diabetes and heart disease combined. According to the Institute of Medicine, the high prevalence of chronic pain suggests that the condition is not being adequately managed. Undertreatment of chronic pain creates large costs to the healthcare system and the U.S. economy; we spend more than $560 billion in the U.S. each year on chronic pain-related healthcare costs. Moreover, chronic pain can carry significant physical and emotional burdens.
The Institute of Medicine has called for a better understanding of the impact of pain in an effort to reduce its toll on the people who suffer from it including the impact on their economic, physical and emotional wellbeing.
Pain Matters seeks to do just that. The documentary explores what chronic pain is, its individual and societal impact, and the future of pain management through the stories and struggles of six individuals living with chronic pain and their loved ones, as well as perspective from leading national experts in pain management. For more information about chronic pain and the documentary, please click here.
Watch the show!
Pain Matters premieres on November 16 and airs again on December 7 and 14.
"Remember..Research is the key to your cure!"
Research Studies Available
Wednesday - December 11, 2013 @ 22:17:49
Research Studies Available!
Dear APF Members,
The Porphyrias Consortium is pleased to let you know that they are enrolling patients in studies for the following diseases. To read more about each study, including eligibility criteria and who to contact, please follow the links below:
A confirmed diagnosis of a porphyria or have a relative who has been diagnosed with a porphyria
If you have not done so already, please join the Porphyria Registry. Joining the Porphyria Registry is crucial in determining the incidence of Porphyria in the United States.
Go to mobile page. ANN ARBOR, Mich. A low level of daily exposure to a common component of sunlight can cause skin damage at the molecular level after just a few days, new University of Michigan Medical School research shows. The findings highlight the need for better sunscreens to protect against these damaging rays, and prevent the process that can cause skin to look old, wrinkled and sagging prematurely. In a new paper published online in JAMA Dermatology, the researchers show that damage starts after just two daily exposures to a low amount of ultraviolet A1, or UVA1, light which makes up most of the UV light we are exposed to throughout the day, and tanning bed light too. Very few of the ingredients in sunscreen products effectively protect against UVA1. The damaging process kept going after further daily exposures. By showing that repeated exposure to the type of UVA1 light that we typically experience on a sunny day causes these damaging processes in the skin, the researchers hope it will lead to the development of new protective ingredients in sunscreens, and more caution about routine sun exposure throughout the day. The study was done by a team from the U-M Department of Dermatology's Photobiology and Aging Skin Research Program, and funded by the National Institutes of Health. The researchers were able to measure the effects of UVA1 at the molecular level using advanced gene expression analysis of skin samples from human volunteers. The researchers shined a low level of pure UVA1 rays, as might be encountered in daily life, on small areas of 22 volunteers' buttocks. A day later, they measured changes in skin pigmentation. Then, they took tiny samples of skin, in order to detect which genes had been 'turned on' by the light exposure. They repeated this process three more times on each participant. After just two exposures, UVA1 rays caused skin cells to make molecules that break down the protein called collagen, which makes skin firm, smooth, and youthful in appearance. The UVA1 also caused the skin to darken a little with each exposure, but this tan didn't protect against further production of the collagen-destroying molecule, called matrix metalloproteinase 1 or MMP1, when the skin was exposed to more doses of UVA1. "Premature skin aging from UV exposure has gotten a lot of attention in the last 10 years, but most researchers have focused on UVB rays, which cause sunburn," says first author Frank Wang, M.D. "But there is very little UVB in sunlight, and most UVB exposure is at midday. During the rest of the day it's mostly UVA, with UVA1 being the majority. UVA1 is also the main component of tanning booth light. So, we wanted to look at whether it can predispose skin to premature aging by simulating repetitive daily exposure. And we found that it can. Furthermore, the mild tanning that occurs does not seem to protect against damage from additional exposures." The study exposed the fair-skinned volunteers in a repeat manner to the amount of UVA1 they would receive in about two hours of strong sun exposure. Statistical analysis showed the pattern of MMP1 production increased progressively with repeated exposure in the majority of patients. A medical dermatologist and assistant professor of dermatology, Wang notes that he often observes the collagen-damaging effects of repetitive sun or tanning booth exposure -- with people in their 20s and 30s coming in for other conditions, but with clear signs of premature aging to their skin. The U-M researchers, led by senior author and lab director Gary Fisher, Ph.D., the Harry Helfman Professor of Molecular Dermatology and Professor of Dermatology, have previously shown similar changes in skin cells from other types of UV light including UVB. However, in contrast with what the researchers had seen with their UVB experiments, the repeated UVA1 exposures didn't suppress the genes that make the molecules that become collagen. The bottom line, they say, is that the new findings suggest a need for new sunscreen ingredients that can protect against UVA1 rays. Currently, only zinc oxide and avobenzone are approved by the U.S. Food and Drug Administration as sunscreen ingredients capable of blocking UVA1. Window glass, and most clothing, also don't necessarily filter out all UVA1. Because UVA1 light from the sun reaches the surface of the earth whenever it's light out, the new research suggests that sunscreen with UVA1-blocking components could be useful throughout the day, not just during the peak sunburn hours of late morning to early afternoon, when UVB is most intense.
Though the current study didn't assess the impact of UVA1 on genetic changes that can lead to skin cancers, other forms of UV are firmly linked to most types of cancerous skin lesions.
"Remember..Research is the key to your cure!"
Global Genes Day
Friday - December 6, 2013 @ 10:30:00
"Remember..Research is the key to your cure!"
Global Genes RARE Project and a host of partners are proud to continue our RARE Webinar Series, a series of educational webcasts this year on relevant and timely topics that should be of interest to the RARE community.
December 11, 2013 11:00 am Pacific Time Register today- space is limited!
With World Rare Disease Day right around the corner (February 28th, 2014), this session will explore event ideas to create awareness for your specific rare disease as well as the entire rare disease community as a whole.
I would encourage you to register and join the discussion. I would also ask that you send this email along to your community and rare friends that might also be interested in the topic.
In 1984 I was hit by a car, and after more than 22 surgeries, nothing has ever been the same. In 1986, I started having problems with ringing in my ears, extreme hearing fluctuation and visual distortions. The symptoms led to a diagnosis of Menieres disease in my right ear in 1986. In 1990 I was diagnosed with Autoimmune Disease, which supposedly had caused the loss of hearing in my left ear. At that time my doctor tried, without success, to treat me with chemotherapy. There was a break in the treatment long enough for me to give birth to my son. I stayed miserably sick during the four long years between chemo and pregnancy. I was finally taken off the chemo treatment after it had eaten my bladder lining.
My appendix was removed unnecessarily while visiting an ER for extreme stomach pain. Actually, I have been to more ERs with abdominal pain than I can count, but other than the time my appendix was removed, there was never any clue as to what might be causing the pain. Over the years Ive heard such explanations as Its just a bad case of gas to There is nothing wrong with you! There were times when I would pray and beg for death, times when I would be so mentally impaired that life had no other meaning cruel harsh hopelessness, times when I could not get out of bed, and times of loneliness when no one could understand what I was going through.
I was finally diagnosed with porphyria two years ago, after being trapped for six hours in a public restroom with severe abdominal pain. I cried out for help to my latest primary care physician, and something clicked for her like it had for no other doctor in my life. After completing two 24-hour urine tests and not knowing what my physician was looking for, I was called into the office and given the diagnosis of Acute Intermittent Porphyria.
My name is Tonya; I was born in Tennessee and raised in Alabama. I am 42 years old and have no known family medical history, as I was adopted at age four. Before I was diagnosed with AIP, I had never heard the word porphyria. However, I have always known that I was different. Even before my porphyria diagnosis, I had many other medical diagnoses on which to blame my strange and many symptoms.
Although the symptoms never really matched the diagnosis, I had the answers, or so I thought. In these two short years, Ive not only learned how to pronounce the word, but I have also learned much about what makes my attacks become active. I still continue to have days and nights where my world is upside down, my pain is unbearable, I cant complete a simple task and loneliness is my constant companion. However, I have gone through the phase of What is Porphyria? and the phase of What does it mean for me? I am now entering the phase of, What can I do to help others? If you would like to contact me in regards to porphyria you may do so by writing to:TCL4U2@aol.com.
Tonya Carpenter-Love
"Remember..Research is the key to your cure!"
Dr. Herbert Bonkovsky speaks about the the Liver & Supplements
Wednesday - November 27, 2013 @ 11:28:34
Charlotte researcher says body-building, fat-burning supplements can cause liver damage
Dr. Herbert Bonkovsky, director of the Liver, Digestive and Metabolic Laboratory at Carolinas Medical Center.
Consuming herbal and dietary supplements for body building or weight loss can lead to serious and sometimes irreversible liver disease or even death, according to a recent study co-authored by a Carolinas Medical Center researcher.
Dr. Herbert Bonkovsky, director of the Liver, Digestive and Metabolic Laboratory at CMC, said people should be careful about taking supplements, which are not regulated as strictly as drugs by the federal Food and Drug Administration.
There needs to be tighter scrutiny and oversight concerning the distribution of these supplements so that consumers understand the dangers associated with them, Bonkovsky said.
Bonkovsky and his colleagues presented their research in November at a meeting of the American Association for the Study of Liver Diseases. It was the largest study of its kind conducted by the national Drug-Induced Liver Injury Network, also called DILIN. The network was created in 2004 to advance research into liver injury caused by prescription and non-prescription medicines, which is the most common cause of acute liver failure.
Bonkovsky, a member of the network since its inception, said researchers have enrolled more than 1,000 patients with all kinds of liver injury due to drugs. That does not include acetaminophen, a common drug sold under brand names including Tylenol. Acetaminophen is the 800-pound gorilla when it comes to liver injury and fatalities, eclipsing all other causes, Bonkovsky said.
About half of all liver failure is caused by acetaminophen. The damage often occurs when someone takes an overdose or when people taking multiple medicines accidentally consume an excessive amount of acetaminophen.
DILIN research has focused on other drugs, including herbal and dietary supplements, which are regulated as foods instead of drugs by the FDA. From 2004 to 2006, such supplements accounted for 4 percent to 6 percent of liver injury cases. But in the past two years, that number has grown to about 16 percent, Bonkovsky said.
Research subjects who reported taking supplements for body building were all men, and most were taking anabolic steroids, he said. The next most common reason for taking supplements was to lose weight. Most of those patients were women taking fat burners, such as green tea extract.
Body-building supplements included certain Oxi-Elite Pro products that were recently recalled by USPlabs after being linked to liver illnesses in Hawaii and other states. One person died, another received a liver transplant, and others are awaiting liver transplants in connection with illnesses induced by the supplements, according to WebMD.
The FDA sent a warning letter to USPlabs recently telling the company to stop distributing products containing the ingredient aegeline, which the FDA said lacks evidence of safety.
Bonkovsky said liver damage caused by supplements can be every bit as severe as that caused by (prescription) drugs.
The take-home message is that these herbals and dietary supplements are not necessarily safe, he said. Theyre not necessarily benign even though theyre marketed as being natural and we all think that natural is safe.
If you have any questions about this post please feel free to read more about Dr. Bonkovsky An APF Expert Doctor. 866-apf-3635.
"Remember..Research is the key to your cure!"
Read more here: http://www.charlotteobserver.com/2013/12/02/4514168/charlotte-researcher-says-body.html#.Up9UfMRDsda#storylink=cpy
In Memory of Ellane Heflin
Sunday - November 24, 2013 @ 10:30:02
The APF is sad to announce that Ellane Heflin, mother of APF Executive Director, Desiree Lyon Howe, passed away Nov 26 in Destin, Florida at age 85. Ms. Heflin, who had AIP, was an APF member since it was founded 31 years ago. To encourage others to participate in porphyria research, Ms. Heflin volunteered as a research patient a number of times since 1982 and volunteered for her last porphyria research project at age 84. She was the oldest person and APF member to participate in porphyria research to date.
She is survived by her children, Elizabeth Ruth Petersen, April Heflin, Deborah Fedele, Dr Joseph Heflin, and Desiree Lyon Howe, and by her grandchildren, Lelia Brougher, Spring Howell, Miranda Dennis, Patrick Petersen, Parker Heflin, Kelsey Heflin, Sarah Taylor and Ian Murdoch, and by her great grandchildren, Elizabeth Brougher, William Brougher, Chloe Mettenbrink, and Gage Mettenbrink and by her sister, Doris Jackson and brother, Louis Workman.
The funeral will take place in Henegar, Alabama on Saturday, November 30, 2013.
We sincerely express our sympathy to Ellane Heflin's family. Memorials and expressions of sympathy in her memory can be sent to the APF, 4900 Woodway Dr, Suite 780, Houston, TX. 77056.
"Remember.Research is the key to your cure"
An Important Message about Panhematin from Desiree Lyons APF Director
It has come to my attention that there is a great deal of misinformation floating around about a new research project with Panhematin . Unfortunately, this misinformation has some truth but is also replete with incorrect assumptions. I am happy to elaborate for any who want to know all about the research. Below is some of the story.
Now for the why hemin/Panhematin is being researched since it has been an effective treatment for decade. Note that the research grant shorn below says for treatment and prevention.. Panhematin is being widely used for prevention of attacks, because many doctors and experts have found it to be highly effective to prevent acute attacks. But that purpose is not on the label. Since it is being used more and more for this purpose , it is important to have research behind it . Some people have very critical attacks that are horribly painful and could be life threatening without treatment. Without Panhematin, I would have died many times. I only wish long ago we would have used it to prevent my attacks.
In addition, the Panhematin label say it is to be used for women with attacks congruent with leuteal phase of the menses. As you all know , it is used for all attacks and in men and women. Therefore, it is important to have this research, too. Therefore, the U.S. Food and Drug Administration just announced it has awarded 15 grants totaling more than $14 million to boost the development of products for patients with rare diseases. Karl Anderson, University of Texas Medical Branch Galveston, Phase 2 Study of Hemin for the Treatment and Prevention of Porphyria Attacksabout $1.5 million over four years. This is actually not much over four years considering the wide range of studies that will be conducted.
Some people are saying that this research is not necessary and that we could and will have heme arginate/Normosang instead. This is not the case. Heme arginate, which has the trade name Normosang, is licensed for use outside the US in a number of countries. Panhematin is only available in the USA unless that is a special request. The APF and Dr. Anderson and other experts tried for many year to get heme arginate to the USA, however, the company would not bring it here. First, there was an issue with the blood bank The blood bank in Finland where it was being manufactured, did not have the requirement of USA blood banks that the FDA required. Also, they would have to spend many millions for research to bring heme arginate here. .
Heme arginate and Panhematin are both owned by Recordati, an Italian Pharma company. Panhematin and heme arginate cost approximately the same Although some feel that heme arginate is more stable, now albumin is being used with both products , not just Panhematin. Seehttp://www.ncbi.nlm.nih.gov/pubmed/1713408 for use. Knowing all of the story is essential before making assumptions where medicine and treatments are concerned There is much more to all of this but the most important issue is that patient volunteers are needed. We sincerely than all who have volunteered YOU ARE THE MEDICAL HEROS DRIVING US CLOSER AND CLOSER TO A CURE . IF YOU ARE WILLING TO PARTICIPATE, PLEASE CONTACT ME AT LYONAPF@AOL.COM. Participant will fly to the University of Texas Medical Branch in Galveston where Dr. Karl Anderson i conducting a number of porphyria research projects. Some of those projects do not require travel but only require your blood and answer questions that are very pertinent to the porphyria research. Many thank, d
"Remember..Research is the key to your cure!"
Holiday Shopping Time! Get your loved ones an American Porphyria Foundation T-Shirt Today!
Friday - November 22, 2013 @ 15:30:01
Want to give your loved one a gift & raise awareness for the American Porphyria Foundation?
American Porphyria Foundation
T-Shirts for SaLE
19.00 Each Includes Shipping ~ Sizes are S, M, LG, XL, 2 XL, 3 XL
PLEASE INCLUDE: I must have name, complete address, and phone number. Also include the Quantity of T-shirts and the size for each one. To accept payment: 1 of 2 options I can accept a VISA/MC only. I must have full name on the card, account#, exp. date, 3 digit code on back of card CVV-.
Your information is kept secure and never shared or put on a list. We can accept will a money order & personal checks. You must have name/address/phone # on them.
For privacy purposes I will be happy to email you the address to send your check or money order to. Once I receive the order I will ship out your product.
All products will be shipped out Priority mail with tracking. Each person will receive a receipt with Purchase.
"Remember..Research is the key to your cure!"
Research Studies Available! Can you or a family member Participate?
The Porphyrias Consortium is pleased to let you know we are enrolling patients in studies for the following diseases. To read more about each study, including eligibility criteria and who to contact, please follow the links below:
A confirmed diagnosis of a porphyria or have a relative who has been diagnosed with a porphyria
We want to keep you informed with the latest news and information. Keeping your contact information up to date can be done quickly and easily on the Web:
The Porphyrias Consortium is a network of physician scientists, and clinical research resources dedicated to conducting clinical research in the Porphyrias. We Can Help You: Become aware of clinical research and clinical trial opportunities; Connect with expert doctors; Get help in managing your disease. Learn More >
The Porphyrias Consortium is a part of the National Institutes of Health's Rare Diseases Clinical Research Network. For more information, visit:www.RareDiseasesNetwork.org
The Rare Diseases Clinical Research Network will make every effort to enroll all the patients we can, but we cannot make any guarantees that we will be able to enroll everyone in a particular study who wants to participate. Participation in research studies is voluntary. Deciding not to participate in a research study does not affect your ability to receive care at any of our Clinical Centers or from other physicians.
The Rare Diseases Clinical Research Network (RDCRN) was established by the National Institutes of Health (NIH) to develop research studies for rare diseases, and to encourage cooperative partnerships among researchers at over 150 clinical centers around the world. This increased cooperation may lead to discoveries that will help treat and perhaps prevent these rare diseases, as well as produce medical advances that will benefit the population in general. The Rare Diseases Clinical Research Network is comprised of a Data Management and Coordinating Center and 17 consortia studying over 100 rare diseases.
The Porphyrias Consortium is a part of NIH Rare Diseases Clinical Research Network (RDCRN). Funding and/or programmatic support for this project has been provided by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and the NIH Office of Rare Diseases Research (ORDR).
The National Institutes of Health does not endorse or recommend any commercial products, processes, or services. The views expressed in written materials or publications do not necessarily reflect the official policies of the Department of Health and Human Services; nor does mention by trade names, commercial practices, or organizations imply endorsement by the U.S. Government.
"Remember..Research is the key to your cure!"
Recordati Rare Diseases, Inc. is committed to providing support to the AIP community.
Tuesday - December 3, 2013 @ 17:14:33
Recordati Rare Diseases, Inc. is committed to providing support to the AIP community.
The Recordati Rare Diseases Reimbursement Support Program is a free service available to patients, caregivers, medical billing staff, healthcare providers, and others who have questions about insurance coverage and reimbursement-related issues including:
For further information, contact the APF: 1.866.APF.3635.
"Remember..Research is the key to your cure!"
Fundraiser Time with Oksana Henn!
Friday - November 22, 2013 @ 10:30:02
Meet AIP Patient Oksana Henn & Her Fundraiser Event
I have AIP diagnosis for over 17 years already. I was diagnosed in Ukraine after I became completely paralyzed (it took me over 10 years to get diagnosed). It took me 2 years to get back up on my feet and functions again. When I moved to USA (Denver, CO) 15 years ago, I found out about Dr. Anderson and went to meet him to confirm my AIP diagnosis. Ever since that time he has been consulting me and my doctors on how to treat my symptoms and what to do with my AIP in general. Some doctors listen to his suggestions, some don't. Those who do not, think that they know more than AIP specialists and try treating me with different medications and methods that actually harm me. We need more doctors like Dr. Anderson, who actually understands and knows AIP and does everything to help patients like me. Over the years my AIP symptoms have been getting worse. Panhematin is the ONLY medication that treat my AIP attacks time and time again. The APF helped me many times with referrals to doctors, suggestions, and just listening to me. APF, thank you very much for everything you do! I have been enrolled in a few AIP research studies over the years. One of them identified the exact gene mutation that I have. This was completely free for me. Another study that is going on now identified my dad as being an AIP gene carrier. This information will help my family (sisters, nieces and nephews) to prevent from being sick for a long time like me. I want to help APF by running a fund raiser on my site. APF is doing a great job educating doctors to be specialized in AIP and other porphyrias. I want this and other fund raisers that I will have to help pay for education for Protect The Future program.
Our health and well being depends on them!
Here is a great FUND RAISER for the American Porphyria Foundation:
50% of all proceeds from sales on the site (below) between now and January 1-st, 2014 will go to American Porphyria Foundation.
Please visit:www.shop.giftbasketmarket.net to order a basket for you and help out your favorite charity! There are different gift baskets for every occasion! Please support the APF & PTF program. Thank you!!!
"Remember..Research is the key to your cure!"
Read about Ruth Taffet
Monday - November 18, 2013 @ 10:30:02
Ruth Taffet
Type of Porphyria:
Acute Intermittent Porphyria (AIP)
I was diagnosed with AIP 45 years ago. My 24 hour quantatative urine was sent to Dr. Watson. The illness began with a ruptured tubular pregnancy. After the operation, I was in extreme pain. I was sent home not being able to retain food or move my bowels and was extremly nauseated. Nine days later the doctor ordered over the phone a triple suppository of compazine. This caused me to faint immediately, and I was rushed to the hospital. My pulse 180, was sent to Booth Memorial in Queens N.Y where they couldn't find out what was wrong, I was given a barium enema, a levine tube, many medications that had disastrous effects, including going into a coma. Fortunately, the doctors that were attending the women in the next bed said, "I know that woman is not crazy." They happened to look in my bedpan and saw red urine. I awoke completly paralyzed. Pins could be stuck all over my body. I couldn't feel anything.
Finally, three months later I was released from the hospital. My hands were shaking, and eventually I couldn't stand the smell of food and was depressed. I was taking a pill that had been killing people in England,. About five years ago, doctors discovered I didn't have any Iron in my bone marrow. Every test proved negative, but in six months of taking iron, my count was normal.
I now have a hemotologist check my blood every six months. Since I had a bout with blisters, I believe I might have HCP. I am eighty years of age, I'm carefull of all medication. I am healthy and only take a mild blood pressure pill. My case was published in the medical journal, Lancet, and was written by Dr. Irwin Cohen in 1962.
"Remember..Research is the key to your cure!"
Do you think to much? Is it Healthy? How to Stop Thinking too Much
It's a golden rule to think before you speak, but you can run into trouble when you think so much that you fail to act, or think yourself into a state of uncontrollable anxiety. Are you looking for a way to stop thinking too much?
Accept that you're thinking too much. Just like eating, thinking is something we need to do to survive, so it is sometimes hard to judge when you are doing too much of it. However, there are several red flags that you are doing too much thinking for your own good. Here are a few of them:
Are you consumed by the same thought over and over again? Are you not making progress by thinking about this particular thing? If so, this may be a sign that you should move on.
Have you analyzed the same situation from a million angles? If you've found toomany ways to look at something before you decide how to act, you may be being counterproductive.
Have you enlisted the help of your twenty closest friends in thinking about a particular thing? If so, then it's time to realize that you can only ask for so many opinions about the same idea before you drive yourself insane.
Are people constantly telling you to stop over-thinking things? Do people tease you for brooding, being a philosopher, or staring out of rainy windows all the time? If so, they may have a point.
2
Meditate. If you feel like you don't know how to stop thinking, you need to learn what it's like to "let go" of your thoughts, so that it's something you can do deliberately.[1]Imagine that thinking is like breathing; you do it all the time, without even realizing it. But if you need to, you can hold your breath. Meditating will help you learn how to release your thoughts.
Just spending 15-20 minutes meditating every morning can make a dramatic impact on your ability to stay in the present and let go of all of your nagging thoughts.
You can also meditate at night to help yourself wind down.
3
Exercise. Running or even walking vigorously can help you take your mind off of all of those annoying thoughts and to focus on your body. Participating in something particularly active, like power yoga or beach volleyball, will have you so focused on your body that you won't have time for your thoughts. Here are some great things to try:
Join a circuit gym. Having to switch to a new machine every minute when you hear that bell ring will keep you from getting lost in your thoughts.
Go hiking. Being around nature and seeing the beauty and stillness around you will keep you more focused on the present moment.
Go swimming. Swimming is such a physical activity that it's even harder to swim and think.
4
Say your ideas out loud. Once you've said everything aloud, even if you're talking to yourself, you've begun the process of letting go. Walk around and pace if you have to. Once you've put your ideas out there, you've begun the process of putting them out into the world and out of your thoughts.
You can say them aloud to yourself, your cat, or to a trusted friend.
5
Ask for advice. You may have exhausted your own thinking power, but someone else might be able to offer a different perspective that makes the decision clearer. This can help let go of your troubling thoughts. Your friend can make you feel better, can ease your problems, and can also make you realize when you're spending way too much time thinking.
Besides, if you're hanging out with a friend, you're not just thinking, right? That's something.
Make a practical list of the things that are troubling you. Whether you're writing on paper or a computer, you should first define a problem, write down your options, and then list the pros and cons for each option. Seeing your thoughts in front of you will also help you stop cycling through them in your head. Once you can't think of anything more to write, your mind has done its job, and it's time to stop thinking.
If making a list still doesn't help you make a decision, don't be afraid to follow your intuition. If two or more options seem equally appealing, thinking more will not make things clearer. This is when you should listen to something deeper.
2
Keep a diary of the things that are troubling you. Instead of lingering over your most persistent thoughts, jot down all of the things on your mind every day. At the end of one week, go over what you've written and make a note of the things that are troubling you the most. You need to deal with those first.
Try to write in your diary at least a few times a week. This will help you get used to the idea of a "thinking time" and will help you sit down with your thoughts, instead of having them trouble you throughout the day.
3
Have a to-do list. Make a list of all the things you have to do on a certain day. Unless "brooding" is on your list of priorities, this will force you to see that you have more important things to do than to sit around pondering the meaning of the universe! The quickest way to organize your thoughts is to put them into something actionable. If you're thinking that you haven't gotten enough sleep lately, make a plan for getting some Z's pronto instead of worrying about it!
The list can be practical and can deal with the bigger things, like: "spend more time with my family."
4
Set a "thinking time" aside for yourself every day. This may sound crazy, but picking a time every day for yourself to worry, wonder, be dreamy, and to get lost in your thoughts can help you control your thoughts in a more productive manner. If you need to, give yourself an hour, say, from 5-6:00 every day. Then, try to get the time down to 5-5:30. If an upsetting thought comes up earlier in the day when it's inconvenient to deal with it, just tell yourself, "I'll worry about that at 5 pm."
This may sound ridiculous, but you've got to try it before you knock it.
1
Solve as many problems as you can. If your problem is that you think too much about nothing, worry for no reason, or think about things you can't control, then there's not much you can do to "solve" the problems that are plaguing your thoughts. But think of the ones you can solve and make an active plan for going about doing so, instead of thinking, thinking, thinking without it going anywhere. Here are some ideas for what you can do:
Instead of thinking about whether or not your crush likes you, take action! Ask him or her out. What's the worst that can happen?
If you're worried that you're falling behind in work or school, make a list of all of the things you can do to succeed. And then do those things!
If you like to think, "What if" a lot, try to do the things that are feasible.
2
Be social. Surrounding yourself with people you love will keep you talking more and thinking less. Make sure to get out of the house at least a few times a week, and make a point of working to develop lasting and meaningful relationships with at least two or three people in your area that you can hang out with. You'll be much more prone to thinking if you spend a lot of time by yourself.
Alone time is definitely a good thing, but it's important to mix up your routine with some time to hang out with your friends, let loose, and have fun.
3
Get a new hobby. Take the time to explore something completely different and out of your comfort zone. A new hobby, no matter what it is, will keep you focused on the task at hand as well as interested in getting results. Don't think that you already know what you like and don't need any more distractions. Trying a new hobby can help you live in the moment and focus on your art, your craft, or whatever. Try some of these:
Write a poem or a short story
Take a night class in history
Take a pottery or ceramics class
Learn karate
Take up surfing
Try biking instead of driving
4
Dance. There are a number of ways to dance -- alone in your room, out at a club with your friends, or even by taking a dance class such as tap, jazz, foxtrot, or swing dancing. Whatever form of dance you encounter, you'll be able to move your body, listen to the lyrics, and live in the moment. It doesn't matter if you're a terrible dancer. In fact, that you would get you even more focused on your dance moves and less focused on all of your niggling thoughts.
Taking up a dance class would be a great way to start a new hobby and to dance.
5
Explore nature. Get outside and start looking at the trees, smelling the roses, and feeling fresh water on your face. That will help you live in the moment, embrace nature and the impermanence of your existence, and to see a world outside of the one you created inside your own head. Put on your sunblock and your sneakers and stop being cooped up in your bedroom.
Even if you're not into hiking, running, biking, or surfing, make a goal of walking through a park at least once or twice a week, taking a weekend trip to something nature-related with your friends during your next vacation, or just going somewhere were you can stare out at a big blue lake or ocean.
And if that seems like too much work for you, just go outside. Being out in the sun will make you happier, healthier, and less likely to brood.
6
Read more. Focusing on the thoughts of other people will not only give you insight, but will keep you from thinking about yourself too much. In fact, reading biographies of inspirational men and women "of action" may inspire you to see that behind every great thought, there is an equally great action. And reading books can also not make you want to do anything except for escape to a new world, which is also nice.
7
Make a gratitude list. Every day, make a list of at least five things you are grateful for. This will make you focus on people and things instead of thoughts. If every day is too much, try doing it every week. Mix it up. Every little thing counts, even the barista who gives you a free refill of your coffee.
8
Appreciate beautiful music. Listening to a great song can make you feel in touch with the world outside your own head. You can do this by going to a concert, playing an old CD in your car, or even getting a record player and some LPs and going old school. Close your eyes, soak in the notes, and live in the now.
It doesn't have to be Mozart or something meaningful or hoity-toity. Listening to Katy Perry can do the trick too!
9
Laugh more. Be around people who make you laugh. Go to a comedy club. Watch a comedy or a TV show with a funny cast that you really like. Watch some funny YouTube videos. Do whatever you have to do to make yourself crack up, toss your head back, and not care about all of the things that are on your mind. Don't underestimate the importance the role of laughter plays in your mental health.
Have you joined rare connect yet? If not please take some time to check it out from around the world all types of people with porphyria coming together to unite.
A 24-year-old man was transferred to the hospital for evaluation of jaundice and abdominal pain. He had a lifelong history of severe photosensitivity and wore long-sleeved shirts and sunscreen to limit sunburn. During the evaluation for abdominal pain, an initial upper endoscopy was negative. However, postendoscopy melena prompted a second look, which revealed multiple mucosal burns caused by the light source of the endoscope during the initial procedure (Panel A). Burns also developed on his fingers from the light source of a pulse oximeter (Panel B). A workup revealed elevated red-cell free protoporphyrin levels and elevated levels of porphyrin in the stool and urine. A diagnosis of erythropoietic protoporphyria was confirmed with genetic testing. Burns are caused by photoactivation of protoporphyrin deposits in tissues. This patient also has severe liver disease due to hepatic protoporphyrin deposition. He is being evaluated for combined liver and bone marrow transplantation.
Global Genes RARE Project and a host of partners are proud to continue our RARE Webinar Series, a series of educational webcasts this year on relevant and timely topics that should be of interest to the RARE community.
December 11, 2013 11:00 am Pacific Time Register today- space is limited!
With World Rare Disease Day right around the corner (February 28th, 2014), this session will explore event ideas to create awareness for your specific rare disease as well as the entire rare disease community as a whole.
I would encourage you to register and join the discussion. I would also ask that you send this email along to your community and rare friends that might also be interested in the topic.
Gary Eysters Donation. Esteemed artist, Gary Eyster, was an APF donor for many years. Thanks to his good friend and APF member, Ralph Grey, Gary also donated his valuable collection of paintings to the APF upon his death. Gary was an innovative, abstract expressionist with studios in Wilmington, North Carolina and York, Pennsylvania. Working until his death in July 2013, Gary never ceased exploring ways to express and fine tune his artistic vision. Garys training spanned the 1950s and 1960s with traditional art education at schools in Philadelphia, Richmond, London, Paris, and Wetzler, Germany. Striving to break away from habits and routines that can stifle creativity, Gary searched for novel ways to introduce spontaneity and randomness into his artistic process. This led him to paint with such unusual objects as plungers, squeegees, wide mouth jars and squeeze bottles. Gary even created a number of works by applying paint and powdered pigments through layers of water to the canvas below. This unique process also allowed him to pull monotype prints from the surface of the water, creating works that were simultaneously unique and derivative of their larger, canvas progenitors.
Garys works were shown in some of the most prestigious galleries and shows in the world. He chose the APF to hold his works to help people with porphyria. He also taught young men and women how to achieve the mastery of some of his techniques and was very interested in the Protect the Future (PTF) program to train future porphyria experts. He understood the great value of present experts sharing their expertise with young doctors as he had shared his talent with young artists. The APF is grateful to Gary for his valuable gift. If you are interested in viewing and /or purchasing these works, please see the website, garyeyster.com. Your purchase will provide funding for the APF PTF and physician education programs. You can also contact the APF to be placed in contact with Ralph Grey, who can assist you with your questions or purchases.
"Remember..Research is the key to your cure!"
Tips for the doctor's office
Saturday - November 2, 2013 @ 10:30:02
Tips for the doctor's office
Make Lists You may not always need to share all of your information with every doctor you see but the following items are particularly important: A list of all of your medications and needed refills, a summary of your medical history, a list of your recent tests, a list of your questions, concerns and new information, forms your doctor needs to address,
Plan Ahead For Your Doctor Visit Prepare your questions and a list of your symptoms, ( For example, racing heart, blisters, etc) Be concise. When you schedule your appointment, ask if you should have test results or other medical records sent to the doctors office before your visit. Nothing is worse than rescheduling for new tests you could have taken earlier or not had with you.
At Your Visit Be on time. Give and expect respect. Bring your lists and tell the doctor what you want to discuss and your goals for the visit. Be as brief as possible. Communication is an especially important skill. Make every word count because the doctor may only have 15 minutes to spend with you.
Be sure you understand what the doctor is advising you. If not, ask questions until you understand. If there is not enough time for all of your questions: Ask for handouts and brochures that will give you more information or schedule another visit.
You and your doctor may have different goals for the visit. For example, your doctor may want to just check your blood pressure, while you may have worries about possible surgery.
Many things can get in the way of helpful communication; emotions, communication style, different goals and lack of time all work against us. When emotions are high, logic is low. If you find that your emotions are interfering with your visit, explain this to your doctor. Try taking a moment to reflect on what you want to say and try again.
Lastly, you may feel that you know more about certain aspects of porphyria than your physician. Major medical journal articles are usually best accepted than internet articles.
After the Visit Often patients have questions they forgot to ask. If it is urgent, call the office right away. Otherwise, check the educational materials to see if the question can be answered there.
If you still dont have the answer, call your doctor. However, it is best to have the question clearly written. Be aware that the doctor may not be able to answer your call until the end of the day, or next business day- but a nurse or physicians assistant may be able to help earlier.
Daylight Savings Time (DST) is nearing its end as colder months fall upon much of the U.S. Instead of long, sunny days, most U.S. states will set their clocks back an hour and enjoy an extra hour of sunlight in the morning but an earlier onset of darkness in the evening.
Daylight saving ends on Nov. 2. Creative Commons
Daylight Savings Time ends on Sunday, Nov. 3, at 2 a.m., when clocks go back to 1 a.m. DST usually ends the final Sunday in October, but this year, it occurs on November's first Sunday.
The extra hour could help some folks catch up on the sleep they lost back in March, when Daylight Savings Time made everyone spring ahead and lose an hour of sleep.
DST was first proposed by entomologist George Vernon Hudson in 1895 as a way to extend daylight hours in summer. But it was adopted as an energy-saving measure by President Franklin D. Roosevelt in the United States and called "War Time," during World War II, from Feb. 9, 1942, to Sept. 30, 1945. The law was enforced 40 days after the bombing of Pearl Harbor.
These days, California and Arizona do not partake in Daylight Savings Time. There are mixed studies as to whether or not the time change actually helps to save energy, Patch.com said.
Those who use personal computers, smartphones, tablets and other electronic devices (just about everyone) dont have to worry about turning the time back because the devices automatically do it. On the first Sunday in November, however, those who do need to manually set the hour hand back should do so before going to bed.
In March, when everyone springs ahead, there are only 23 hours in the day. But when most of the country falls behind next month, there will be 25 hours in the day. What will you do with the extra hour?
"Remember.Research is the key to your cure!"
NEW Caretaker Support Forum.
Sunday - October 27, 2013 @ 18:44:02
NEW Caretaker Support Forum.
Warren Hudson, who serves on the APF Board of Directors, has agreed to head our Caretaker Support Forum for spouses or partners who help their loved one cope with porphyria. To read more about Warrens story as a caretaker for a loved one with AIP view here.
The Caregiver Support Group strives to provide a forum to ask questions, share advice, experiences and provide a sounding board for those going through similar circumstances.
Our goal is to eventually provide multiple resources to assist caregivers in their day-to-day lives. This is your community and your input will help shape this service. Whether you are a spouse, partner, relative or friend of a porphyria patient, we want to hear from you. Contact the American Porphyria Foundation or email us at apfcaregiver@aol.com for more information.
We respectfully request that only caregivers of patients in the active process of diagnosis or with a diagnosis of a porphyria participate in this group.
8 Important Ongoing Research Projects that need your help
The Apf is currently involved in helping recruit diagnosed Porphyria Patients of all types. We need your help to make these studies a success. Many of the studies do not require any travel, and for some of them the travel will be provided. You can read about the ongoing studies by going to the Porphyria Research Consortium section on the Rare Disease Research Networks website.
If you haven't already please join the Porphyria Registry while you are there. It only takes a few minutes and it will help more than we can express.
"Remember. Research is the key to your cure!"
Reminders about finding a good APF Doctor for YOU
Thursday - October 24, 2013 @ 10:30:02
The American Porphyria Foundation promotes comprehensive care necessary for treating individuals with Porphyria. This section of our website offers suggestions for finding a local doctor who can manage your Porphyria, options for having your doctor consult a Porphyria specialist, and information on arranging a visit to a Porphyria clinic.
Because Porphyria is so rare, few physicians have experience treating patients with the disease. Most patients are in fact treated But the APF can help by putting your doctor's office in touch with a Porphyria specialist who can offer guidance on your care.
For those who need a diagnosis, you may be able to obtain a consultation at Porphyria clinic. Call the APF to reach a porphyria expert at a porphyria center. The APF office will also guide you to doctors who are not experts but are knowledgeable about porphyria. You may be asked to send your blood, urine, and stool samples for evaluation in advance of a clinic appointment. Especially if you plan to travel for a consultation, it is a good idea to call ahead and explain that you would like to be evaluated for Porphyria so that you can be sure you have done any necessary testing in advance. If local video conferencing facilities are available, telemedicine consultation with a Porphyria expert is also available.
Regardless of your situation, it is best to establish a good relationship with a doctor in your area. Developing a relationship with a primary care physician takes time and can be frustrating, particularly when you have difficulty finding a doctor who will manage your care. In this section of the website, you will also find Tips for the Doctor's Office that may help.
If you're having trouble finding a local doctor, the following organizations' doctor finder or physician referral services could be helpful. The APF does not recommend or endorse the doctors listed through these sites.
If you would like to read about supporting programs to ensure the quality of specialists in the field of porphyria, please see our Protect Our Future campaign information.
"Remember.Research is the key to your cure!"
Family Involvement with the Caretaker Support Forum~Please Join
Monday - October 21, 2013 @ 10:30:04
Caretaker Support Forum
New APF Caretaker Support Forum "Please get involved with your family, you may save there life, with encouragement, understanding, knowledge, Doctors experience"~ Purple Light
Warren Hudson, who serves on the APF Board of Directors, has agreed to head our Caretaker Support Forumfor spouses or partners who help their loved one cope with porphyria. To read more about Warrens story as a caretaker for a loved one with AIP click here.
The Caregiver Support Group strives to provide a forum to ask questions, share advice, experiences and provide a sounding board for those going through similar circumstances.
Our goal is to eventually provide multiple resources to assist caregivers in their day-to-day lives. This is your community and your input will help shape this service. Whether you are a spouse, partner, relative or friend of a porphyria patient, we want to hear from you. Contact the American Porphyria Foundation or email us at apfcaregiver@aol.com for more information.
We respectfully request that only caregivers of patients in the active process of diagnosis or with a diagnosis of a porphyria participate in this group.
Remember.Research is the key to your cure!"
Doris Stevens Letter about VP
Saturday - October 19, 2013 @ 10:30:00
Doris Stevens
Type of Porphyria:
Variegate Porphyria (VP)
Doris's Letter to Porphyria
DEAR JOHN: For therapy, a caring doctor had recommended I write about my illness, that I state what it has done to me and how it has affected my life and finally, what I hope will happen no matter how unrealistic. Since it took a better part of my lifetime to unravel the mysterious maladies that plagued me most of my life, it was difficult to write about it in a less compassionate form. It is important to understand when you read this that it is possible to have been born with more than one congenital anomaly. In my case, I was born with a mild Arnold Chiari Malformation which accounts for an inability to nurse, dizziness and clumsiness in infancy and adolescence. Porphyria symptoms were not present until my early to mid-teens. I am sorry to inform you that I have never loved you. I have truly never understood you and even worse, no one else has understood you either! Starting from my earliest memories you have caused confusion and misunderstanding. You caused my parents to believe I was ill mannered at the table. Because of this I spent unspeakably cruel hours sitting at the dinner table being disciplined, eating my own regurgitated food, uncountable hours of stomach upsets, pain and tears. My mother always believed I personally rejected her since I couldn't nurse, and believed I rejected her excellent cooking efforts from the beginning of my existence. By the time I was 10, I was labeled a hypochondriac and clumsy. All this due to my dizziness, chronic mild aches and pains and chronic cramping constipation. My complaints were stonewalled. I learned to bury you. Anything was possible. I could fight you. You and my parents made me strong, the physical pain from life's normal upsets meant nothing to me. I concentrated on being the best at school, my uncontrollable mood swings hampered my social life until I conquered that too. Occasionally throughout my adult life you would dig yourself out of your grave and I would be desperate enough to seek out Dr. Exorcist only to relive the cycle of my youth. Sometimes he would refer me to Mack the Knife, Dr. Pill Happy and Dr. Nightmare. Most of the time this proved to be a bad choice. But, this was back when I didn't realize I had a choice. I was naive enough to believe exorcism always worked and to not obey Dr. Pill Happy was unthinkable. You taught me to dance between the rain drops. I concentrated on family, college, and a successful career. Once I passed 40, the rain storm started becoming more constant, the space between the drops became smaller and smaller. Until I reached the day when my plodding dance steps were so limited that my family could take it no longer and forcibly placed me in a wheelchair. I learned what it was like to be short and invisible. I had limited cognizance, would blank out (grand mall siezures), lose my balance, get severe flu like symptoms, severe back, shoulder, neck and all over pain and migraines, and the list goes on. I lost my business, some friends, and hold on loving life. I learned what it was like to truly wish for death. I became desperate and even more desperate while the Dr. Mack's argued over the semantics of my illness. This is where I learned that you and I had been together since birth. What a wonderful feeling to have been vindicated and to have been healed! Dr. Mack could be a good guy after all. I cut you out of my life, but experienced the most devastating blow to discover a month after Dr. Mack's handiwork, while having a wellness celebration or farewell BBQ party about you, that you had an evil twin (according to an unsurprised Dr. Mack the Knife), yet to be named. Fortunately your twin is not identical, but is definitely a Gemini, unpredictable. He's thought to be a rarity. I can remember the feeling of morning. A bright new day, the delicate warmth of sunshine bathing my face, the sound of birds chirping, a smell and feel of morning air through the crack in the window, the feeling of warmth and strength flowing through my body, the excitement of a whole day ahead of me to attack and enjoy life. It seems like only yesterday that I would take my nature walks with friends, challenging ourselves to exceedingly longer and longer jog-walks each day. Building a sand castle at the beach, standing in the sun watching a parade, going outdoors on a hot sunny day, an outdoor BBQ, going to a day game at the stadium, walking my dog around the block, wandering through the grocery store taking goods off the shelf, standing at the stove long enough to cook something, taking a long drive, playing chase with my little dog, the satisfaction of scrubbing a dirty rental house clean, cleaning my own house, gardening, working as I choose, doing all these things I took for granted would last my lifetime. The excitement of seeing snow on the mountains and planning a ski trip still haunts me. I will never do that again is my slogan for today. Focusing on what I can do is my personal challenge. Now if I have slept, I wake to the feeling of burning pain everywhere I can feel my body. If I concentrate very hard I can hear a bird chirp over the loud ringing in my head, my nose is too plugged to smell my own bad breath let alone the morning breeze, and if I roll carefully off the bed I may not feel a jolt of excruciating back or leg pain. If I awake with any energy it is a blessing I savour for the few hours it may last. Sometimes I truly dread a walk from here to there. The gentle warmth of the sun has become a seering pain to me that evokes a headache, nausea, stomach pain, and more. I am almost always hot and have flashes burning up all day and night. Feeling cold is a blessing. The heat from the sun can trigger such a violent reaction that even the vision in my right eyes spasms and fails. I live with constant pain, fear of eating the wrong thing, hoping I will be able to sleep when the time comes and counting the physical things I can no longer do as a regrettably growing list. Out of the blue my heart will thump, bump and race for what seems an eternity. The head ringing often becomes loudly unbearable. I have learned to surround myself with noise to keep from going mad. Even worse is the unwanted knowledge about my body that keeps flowing in. I spent a lifetime bearing you and burying you. I spent 20 years trying to find out why these things are happening and now the why's won't stop. The list of diagnoses and pills/things I am allergic too is too long for me to remember. I usually just list the highlights on medical forms. You make me feel like a freak of nature. Dear John, the evil twin, I want you to move out. I want to hear silence, I want to walk my dog in the sun and build a sand castle at the beach with my granddaughter. I want to hop out of bed and go grocery shopping unassisted. I want to learn to love the things I have learned to hate because of you. I want to go dancing in the evening and clean my house during the day. I want to walk ten miles on a summer day. I want to be able to eat like anyone else and not have pain, gain weight or get sick. I want to be able to toast the New Year. I don't care about my career, it is gone along with my total naivity about humanity. Most of all, I never want to have to see your friends, Dr. Exorcist, Dr. Pill Happy, Dr. Nightmare and Dr. Mack the Knife again as long as I live. I want to feel the morning! Me P.S: John, I have often been asked to write about you and to attempt this had caused me to be unbearable to live with for days, but a Dear John letter was a very pleasant task.
Remember.Research is the key to your cure!"
What is a Ferritin Test and why is it import to have it checked when you have Porphyria
Thursday - October 17, 2013 @ 10:48:49
A ferritin test measures the amount of ferritin in your blood. Ferritin is a blood cell protein that contains iron. A ferritin test helps your doctor understand how much iron your body is storing.
If a ferritin test reveals that your blood ferritin level is lower than normal, it indicates your body's iron stores are low and you have iron deficiency.
If a ferritin test shows higher than normal levels, it could indicate that you have a condition that causes your body to store too much iron. It could also point to liver disease, rheumatoid arthritis, other inflammatory conditions or hyperthyroidism. Some types of cancer also may cause your blood ferritin level to be high.
You may have a ferritin test for several reasons:
To diagnose a medical condition. Your doctor may suggest a ferritin test if other blood tests have shown that the level of oxygen-carrying protein in your red blood cells (hemoglobin) is low, or if the proportion of red blood cells to the fluid component in your blood (hematocrit) is low. These may indicate that you have iron deficiency anemia. A ferritin test can help confirm that diagnosis.
A ferritin test may also be used to help diagnose conditions such as hemochromatosis, liver disease and adult Still's disease, among others.
When used to diagnose a medical condition, a ferritin test may be done in conjunction with an iron test and a total iron-binding capacity (TIBC) and transferrin test. These tests provide additional information about how much iron is in your body.
To monitor a medical condition. If you've been diagnosed with a disorder that results in too much iron in your body, such as hemochromatosis or hemosiderosis, your doctor may use a ferritin test to monitor your condition and guide treatment.
If your blood sample is being tested only for ferritin, you can eat and drink normally before the test. If your blood sample will be used for additional tests, you may need to fast for a certain amount of time before the test. Your doctor will give you specific instructions.
During the ferritin test, a member of your health care team takes a sample of blood by inserting a needle into a vein in your arm. The blood sample is sent to a lab for analysis. You can return to your usual activities immediately.
The normal range for blood ferritin is:
For men, 24 to 336 nanograms per milliliter (standard units) or 24 to 336 micrograms per liter (international units)
For women, 11 to 307 nanograms per milliliter (standard units) or 11 to 307 micrograms per liter (international units)
Lower than normal results A lower than normal ferritin level indicates that you have iron deficiency. You may also be anemic. If your ferritin level is low, your doctor will work to determine the cause.
Higher than normal results A higher than normal ferritin level can be caused by:
Hemochromatosis A condition that causes your body to absorb too much iron from the food you eat
Porphyria A group of disorders caused by an enzyme deficiency that affects your nervous system and skin
Rheumatoid arthritis, adult Still's disease or another chronic inflammatory disorder
Liver disease
Hyperthyroidism
Type 2 diabetes
Leukemia
Hodgkin's lymphoma
Multiple blood transfusions
If your ferritin level is above normal, your doctor may need to evaluate the results along with those of other tests to determine next steps.
For specifics about what your ferritin test results mean, talk to your doctor. Notice in the end it mentions Porphyria. As an AIP patient myself I have it checked by my Doctor once or twice a year. So may need it more or less depending on their circumstances so if you have questions print this out and bring to your next Doctors Visit.-Purple LIght
Rememberâ?¦..Research is the key to your cure!
Important message ~ National Porphyria Registry
Wednesday - October 16, 2013 @ 10:30:04
Important Notice
Porphyria experts have created a National Porphyria Registry-a type of partnership between the porphyria experts and YOU as a way to share information about YOUR health and treatment. Also, it is the best means to determine the incidence of porphyria and prove that there are enough porphyria patients who want improved health care to warrant government funding. If we don't speak up, we will be left behind when research grants are presented. Please join the registry!
Joining the Porphyria Registry is anonymous, and there is no cost to you. All data will be stored in a secure, computerized database. No personal identifying information will be given to anyone without your expressed approval. Please note that joining the Registry is not the same action as joining the APF.
To better understand National Registries, you can attend the following webinar on Oct 23, 2013.
Biofeedback is a technique you can use to learn to control your body's functions, such as your heart rate. With biofeedback, you're connected to electrical sensors that help you receive information (feedback) about your body (bio). This feedback helps you focus on making subtle changes in your body, such as relaxing certain muscles, to achieve the results you want, such as reducing pain.
Biofeedback helped me greatly when suffering daily pain and Porphyria it may help you ask your Doctor about it.
In essence, biofeedback gives you the power to use your thoughts to control your body, often to help with a health condition or physical performance. Biofeedback is often used as a relaxation technique.
Biofeedback, sometimes called biofeedback training, is used to help manage many physical and mental health issues, including:
Anxiety or stress
Asthma
Chemotherapy side effects
Chronic pain
Constipation
High blood pressure
Incontinence
Irritable bowel syndrome
Raynaud's disease
Biofeedback appeals to people for a variety of reasons:
It's noninvasive.
It may reduce or eliminate the need for medications.
It may be a treatment alternative for those who can't tolerate medications.
It may be an option when medications haven't worked well.
It may be an alternative to medications for some conditions during pregnancy.
It helps people take charge of their health.
Biofeedback is generally safe. Biofeedback may not be appropriate for everyone, though. Be sure to discuss it with your doctor first.
During a biofeedback session, a therapist attaches electrical sensors to different parts of your body. These sensors monitor your body's physiological state, such as brain waves, skin temperature or muscle tension. This information is fed back to you via cues, such as a beeping sound or a flashing light. The feedback teaches you to change or control your body's physiological reactions by changing your thoughts, emotions or behavior. In turn, this can help the condition for which you sought treatment.
For instance, biofeedback can pinpoint tense muscles that are causing headaches. You then learn how to invoke positive physical changes in your body, such as relaxing those specific muscles, to reduce your pain. The ultimate goal with biofeedback is to learn to use these techniques at home on your own.
A typical biofeedback session lasts 30 to 60 minutes. The length and number of sessions are determined by your condition and how quickly you learn to control your physical responses. You may need a series of 10 sessions or as many as 50, which can make it more expensive and time-consuming. Biofeedback is often not covered by insurance.
Types of biofeedback Your therapist may use several different biofeedback techniques. Determining the technique that's right for you depends on your health problems and goals. Biofeedback techniques include:
Electromyography (EMG) biofeedback. This type gives you information about your body's muscle tension so that you can practice relaxation.
Temperature (thermal) biofeedback. Sensors attached to your fingers or feet measure your skin temperature. Because your temperature often drops when you're under stress, a low reading can prompt you to begin relaxation techniques.
Galvanic skin response training. Sensors measure the activity of your sweat glands and the amount of perspiration on your skin, alerting you to anxiety.
Heart rate variability biofeedback. This type of biofeedback helps you control your heart rate in an effort to improve blood pressure, lung function, and stress and anxiety.
Biofeedback devices You can receive biofeedback training in physical therapy clinics, medical centers and hospitals. But a growing number of biofeedback devices and programs are being marketed for home use. Some of these are hand-held portable devices, while others connect to your computer. You can try different devices until you find one that works for you, or ask your doctor for advice. Check with your health insurance company to see what costs, if any, associated with biofeedback devices are covered.
Be aware that some products marketed as biofeedback devices may not be, and that not all biofeedback practitioners are reputable. If a manufacturer or biofeedback practitioner claims that a biofeedback device can assess your organs for disease, find impurities in your blood, cure your condition or send signals into your body, check with your doctor before using it, as it may not be legitimate. Experts aren't entirely sure how biofeedback works. But if biofeedback is successful for you, it may help you control symptoms of your condition or reduce the amount of medication you take. Eventually, you can practice the biofeedback techniques you learn on your own.
Stress is a normal psychological and physical reaction to the ever increasing demands of life. Surveys show that most Americans experience challenges with stress at some point during the year. In looking at the causes of stress, remember that your brain comes hard-wired with an alarm system for your protection. When your brain perceives a threat, it signals your body to release a burst of hormones to fuel your capacity for a response. This has been labeled the "fight-or-flight" response. Once the threat is gone, your body is meant to return to a normal relaxed state. Unfortunately, the nonstop stress of modern life means that your alarm system rarely shuts off.
That's why stress management is so important. Stress management gives you a range of tools to reset your alarm system. Without stress management, all too often your body is always on high alert. Over time, high levels of stress lead to serious health problems. Don't wait until stress has a negative impact on your health, relationships or quality of life. Start practicing a range of stress management techniques today.
Do you know anyone who isn't at times stressed out these days? The pace of modern life makes stress management a necessary skill for everyone. Many people juggle multiple responsibilities, work, home life, caregiving and relationships. Learning to identify problems and implement solutions is the key to successful stress reduction.
The first step in successful stress relief is deciding to make a change in how you manage stress. The next step is identifying your stress triggers. Some causes of stress are obvious job pressures, relationship problems or financial difficulties. But daily hassles and demands, such as commuting, arranging day care or being overcommitted at work, can also contribute to your stress level. Positive events also can be stressful. If you got married, started a new job and bought a new house in the same year, you could have a high stress level. While negative events in general are more stressful, be sure to also assess positive changes in your life.
Once you've identified your stress triggers, you can start thinking about strategies for dealing with them. Sometimes the solution may be as easy as turning off the TV when the evening news is too distressing. Or, when you can't avoid a stressful situation, try brainstorming ways to reduce the irritation factor. And don't feel like you have to figure it out all on your own. Seek help and support from family and friends. You may want to ask them what stress-relief techniques have worked well for them. And many people benefit from daily practice of stress reduction techniques, such as mindfulness, tai chi, yoga, meditation or being in nature.
Stress won't disappear from your life. And stress management isn't an overnight cure. But with practice, you can learn to manage your stress level and increase your ability to cope with life's challenges.
Relaxation techniques are an essential part of stress management. If you're an overachiever, you may put relaxation low on your priority list. Don't shortchange yourself. There are active ways of achieving relaxation. Relaxation is invaluable for maintaining your health and well-being, and repairing the toll that stress takes on your mind and body.
Almost everyone can benefit from learning relaxation techniques. Relaxation techniques help to slow your breathing and to focus your attention on the here and now. The concept of enjoying the moment we are living in, rather than being worried about what could happen in the future. Common relaxation techniques include meditation, mindfulness, tai chi and yoga. For a more active approach, walking outdoors or participating in a sporting sports activity can be relaxing.
It doesn't matter which relaxation technique you choose. What matters is that you select a technique that works for you and that you practice achieving relaxation regularly.
Rememberâ?¦..Research is the key to your cure!
AIP my weekend experience as we speak
Saturday - October 12, 2013 @ 12:58:45
So today I thought I would blog about my experience Sat and Sunday Today. As many of you know I have AIP. My symptoms change just as the weather changes. The older I get the different each "Purple People Eater Attack" gets it, it sets me back. As of late their has been some major problems with getting medications to help me and admitting me into the hospitals even for glucose, and Panhematin. I don't even ask for pain meds, but these problems we have been at battle again for the last 4 months. Back to my story, So yesterday my day started out so slow, I was sick to my stomach I thought I was hungry so I got my food, not hungry still ate my food. 1/2 hour later in bed sick, just feeling like im going down hill fast, so I take my dogs for a walk to try to block the pain and the feeling I have. For dinner I went old school good ole fashioned Mac & Cheese that seemed to keep me at bay. At the same time as I was just pretending nothing was wrong more intense pain came and gone. Watching the ALCS baseball game game 1 go Tigers! Then won and went to bed. My dogs were just watching me through the night and coming up to me, toss and turn, get into the fetal position and my back and legs are on fire, im hot and then its like I progress to be in a no sleep mode. I wake up to the pain I know its there and cant ignore it, I get ready for my important meeting Sunday morning, evidently could not hold the dinner from last night down not once, twice but three times, i cant think now im in trouble. I've called the Dr. on a Sunday and left a message with the RN there its a good hospital. 11:30 am im sitting in this meeting and it just comes from the back around the right side like someone stabbing me over and over my head hurts im shaking what do I do in front of 150 people? I try to ignore it 1/2 later I left the meeting and ate carbs and now im writing in pain. Do you think anyone notices that im in that much pain I want to cry it hurts so bad, but someone has the nerve and says whats your problem? I said im not feeling well at that moment I could ring someones neck because they dont understand I dont expect them to but at that moment panic sets in.. So I tell you my honest experience at this very moment that the pain and disease are real, there is a real need for Drs to get together and talk more out of the box about Porphyria and be aware of what needs to be done. Do what you can to get through it and be determined to get help and quickly. Im still waiting for the two hospitals call me back to get me in so what do I do in the meantime? Have you been there, live in fear, I could get really angry but what is the point? I do the best I can during this difficult time and pray it will pass soon. Keep positive, stay strong endure, I know its not easy and we know what will really help us, my point is to get involved with research projects, listen learn and speak up. Now back to resting.. Rememberâ?¦..Research is the key to your cure!
Sleeping with Sinus pain & congestion with Porphyria
Wednesday - October 9, 2013 @ 12:56:28
Not sleeping well affects both your body and your mood, but when you have sinus pain and congestion, getting a good nights sleep may be easier said than done. The sinuses are empty cavities that reside within the cheekbones, around the eyes, and behind the nose. They warm, moisten, and filter air into the nasal cavity. A sinus infection or sinusitis occurs when there is swelling in the nasal sinuses and passages. You may feel symptoms like pressure around the nose, eyes or forehead, a stuffed-up nose, and thick mucus. Some people also report tooth pain with sinusitis. And if you have allergies, you are at greater risk for sinus trouble, according to The American Academy of Allergy, Asthma & Immunology. There are many reasons that sinus pain and congestion get worse at night. One is that allergies tend to be worse at night, and two, is that when you lie down, your nose becomes more congested, says Jordan S. Josephson, MD, an ear, nose, and throat specialist at Lenox Hill Hospital in New York City and the author of Sinus Relief Now. But this doesnt mean you should give up on a good nights sleep. Instead, try these expert-approved tips to help sleep better with sinus pain and congestion: 1. Take an antihistamine before bed. If you have allergies, taking an antihistamine before bed can help control your sneezing and runny nose, Dr. Josephson says. Some antihistamines make you sleepy in addition to keeping allergy symptoms at bay, so its a win-win. If you use a nasal spray for your allergies, you can try using that at night, too, adds Satish Govindaraj, MD, an assistant professor of otolaryngology at Mount Sinai Hospital in New York City. Check the Acute Drug Safety List First 2. Make your bedroom a pet-free zone. Allergies can make sinus pain and congestion worse. If you have an allergy to dust mites or to pets, keep your bedroom as free from allergens as possible, says Dr. Govindaraj. Keep your pet out of the bedroom, and consider investing in dust-proof covers for your pillows and comforters. 3. Prop up your head. For congestion relief, sleep with your head elevated on a few pillows and maintain a position where your head is above your heart, suggests Govindaraj. This will decrease blood flow pooling in the nose. Lying flat, by contrast, allows mucus to build up in your sinuses, where it can clog your nasal passages and disrupt sleep. 4. Skip that nightcap. You may think that a glass of wine before you turn in will help with sleep, but that is a myth especially if you have sinus pain and congestion. Alcohol can make you feel congested, especially wine, says Govindaraj. If you are prone to sinus pain or congestion, dont drink alcohol before bed. Alcohol can also leave you feeling dehydrated, which can aggravate sinus pain. 5. Avoid caffeine before bed. This is especially important, Josephson says. Caffeine is a stimulant that will keep you awake, so it makes sense to cut it off before 2 p.m. Also, caffeine is dehydrating, so it will make your sinus pain and congestion worse. Instead, choose water or decaffeinated and herbal teas in the afternoon and evening to quench your thirst. 6. Keep nasal passages moist. During the day, use a simple over-the-counter nasal saline spray to keep nasal passages clear, or rinse your sinuses with a neti pot. At night, using a humidifier can help to avoid drying out the air, especially during the winter, says Sam S. Rizk, MD, a New York City-based ear, nose, and throat doctor and facial plastic surgeon. 7. Keep your bedroom cool and dark. This is good advice for anyone with problems sleeping, including people with sinus pain. Other sleep hygiene tips from the National Sleep Foundation include maintaining a regular bed and wake time (even on weekends), using your bedroom only for sleep and sex, and avoiding any stressful activities before bed. 8. Know when to call the doctor. If you have severe congestion and sinus pain for a week or more and have an accompanying fever, you should see an otolaryngologist [an ear, nose, and throat specialist] because it could be a sign that you have a sinus infection that requires more aggressive treatment, Dr. Rizk says.
By following these tips, you can sleep better and get the congestion relief, but when you have sinus pain and congestion, getting a good nights sleep may be easier said than done.
Rememberâ?¦..Research is the key to your cure!
Discussing AIP with Your Family
Wednesday - October 9, 2013 @ 09:33:38
Discussing AIP with Your Family
For many people, a diagnosis of Acute Intermittent Porphyria (AIP) brings a long journey of not knowing to an end. But living with AIP begins another journey. Your family can be a key partner in helping you to manage the disorder. This discussion guide was designed to help you talk about AIP with your family. Here are some questions you may be asked and some tips for answering those questions. What is AIP? Explain to your family that AIP is a rare inherited disorder that involves a lack of one of the enzymes needed to make heme. Heme is the oxygen-carrying component of red blood cells and is vital for all of the bodys organs.1 Because it is genetic, your family members may want to think about talking with their doctors about genetic testing. Also, let them know that many people who are predisposed to the disorder may never experience an attack. Why does AIP cause symptoms like pain and muscle weakness? Your family may already be familiar with the symptoms of the attacks that characterize AIP, particularly if they have lived with you through an attack. In fact, giving a name to the disorder that has affected you may help them understand what you have experienced. Explain that an attack is associated with an overproduction and abnormal buildup of chemicals called porphyrins or porphyrin precursors. These chemicals normally do not build up in the body. How this leads to specific symptoms is not known. What can we do? If your family has been impacted by the symptoms you have experienced, you can empower them by allowing them to be a part of your AIP management. Tell them about the triggers that may be associated with attacks. This may be particularly important if members of your family smoke or if part of your family culture includes drinking alcoholic beverages. Make sure your family understands that severe dieting or carbohydrate restrictive diets are not advised for people with AIP, because they may stimulate the production of porphyrins. Is there treatment for AIP? Because AIP is a condition that can result in sporadic attacks, it is important to think of treatment as a management plan, rather than as something to be handled solely by being given medication by your doctor. With the help of your doctor, you may be able to identify certain triggers of attacks which you will want to address. For example, for some people attacks can be triggered by severe dieting or carbohydrate restrictive diets or use of some medications.
Rememberâ?¦..Research is the key to your cure!
An amazing life journey with James Beadle and EPP
Friday - October 4, 2013 @ 16:12:03
James Beadles
Type of Porphyria:
Erythropoietic Protoporphyria (EPP)
I live life with EPP! I was diagnosed when I was six by a dermatologist named Carl Anderson who has since passed away. Up until my diagnosis, my parents had heard it all from a number of doctors. I was allergic to a medicine, or I was allergic to weed killer, to simply saying, "it is just a rash." All the while, I would scream in pain. My parents would help by placing cool clothes on me.
I live in sunny southern California in a beach town. All my friends were into surfing and sailing. The outdoors is part of life in SoCal. I did not let my EPP stop me from enjoying the outdoors though sometimes I paid dearly. I played baseball until high school. I learned to sail. I ran in triathlons and half-marathons. I snow skied and water-skied. I played golf. All the time I endured the funny looks and mean things said about the way I looked and had to dress. I did not let it stop me. Sure, it bothered me when I was young. It hurt. However, as I got older I saw it as other people's problem, not mine. I was living my life the best way I knew how. I was not going to let EPP stop me from enjoying life.
I had a doctor once who told my parents I should move to Seattle where it was cloudy more often. He said I should learn to play chess and ping-pongindoor sports instead of baseball and golf and sailing. My parents would hear nothing of it; they knew I was going to live my life the way I wanted to live.
I have had two liver transplants because of my EPP. The porphyrins dumped into the liver and made it cirrhotic. I had my first transplant when I was 27 years old. The liver lasted 12 years, during which I was able to continue my normal active lifestyle. I married and had two kids. Neither of my kids shows symptoms of EPP. In fact, one wants to be a lifeguard! Both of my children can run around on the beach all day without being burned, well, aside from basic sunburn. Their mother and I lather them with sunscreen when they go out to the beach or are playing soccer or swimming. The boys are six and eight and I am confident they do not have EPP.
My second transplant was more dramatic. I was 39, my liver and kidneys failed, and I went into a coma. I was transplanted three weeks later and subsequently spent the next eight months in UCLA Medical Center. I was on dialysis for six months after which by some miracle my kidneys began to work again. The transplant and hospitalization took a great toll on my body. I am no longer able to be as active as I was. I have neuropathy in my feet from the kidney failure and nerve damage from being in bed for so long. I am twenty pounds underweight and weak. I like to joke that I am a 42-year old living in a 92-year-old body. I still live with the EPP and who knows how long this liver will last. I take infusions of Panhematin to slow the progression of porphyrins into the liver (this is the hope anyway). The key is I am still living.
I still endure the looks from people, like the other parents at the soccer field when I watch my kids play. I do not care if they think it is odd someone wearing long pants, long sleeves and gloves on a 90-degree SoCal day. To me, they have a problem, not me. People do what they have to do to cope. I am not going to let EPP keep me from enjoying my life and enjoying watching my kids grow up. My kids understand that Dad has to be careful of the sun. They understand Dad is not as strong as he once was because of his surgery. They understand why Dad has to wear protective clothing in the pool; they are just happy that Dad is in the pool with them! Grown-ups should be so understanding.
I hope you enjoy my story and I am anxious to hear how others with EPP are LIVING, not just coping or suffering. Someday there will be a cure for this, and I plan on being around to see it!
Rememberâ?¦..Research is the key to your cure!
Fall Time
Thursday - October 3, 2013 @ 11:45:39
Have a happy fall- fun- filled weekend to everyone!
Rememberâ?¦..Research is the key to your cure!
Porphyria and background resources
Tuesday - October 1, 2013 @ 14:07:50
Background
Porphyria is named from the ancient Greek word porphura, meaning purple.[1] Porphyrins are precursors of heme, a part of the hemoglobin molecule. Heme is manufactured in a multistep process. Defects of enzymes needed at various steps of heme synthesis result in distinct clinical syndromes known as porphyrias. These syndromes can be clinically classified into those predominantly involving the skin, those manifesting as disorders of the liver/nervous system, and a combination involving all 3 entities (see the image below). Clinical classification of porphyrias. Porphyrias can be inherited or (rarely) acquired.[2] With the exception of congenital erythropoietic porphyria (CEP), which is autosomal recessive, all other porphyrias are inherited as autosomal dominant disorders. They invariably result in accumulation and increased excretion of porphyrins and their precursors. Some porphyrias have acute presentations (acute intermittent, variegate, hereditary coproporphyria), whereas others have a chronic, relatively stable presentation (congenital, erythropoietic).[3] King George III of England had symptoms of abdominal pain, rashes, reddish urine, and psychotic episodes that are consistent with porphyria, although the account is disputed by many.[4] During the period 1955-1959, approximately 4000 people in southeast Anatolia (Turkey) developed porphyria due to the ingestion of hexachlorobenzene (HCB), a fungicide that was added to wheat seedlings.[5]
Champe PC, Harvey RA, eds. Conversion of amino acids to specialized products. Biochemistry. 2nd ed. Philadelphia, Pa: Lippincott, Williams & Wilkins; 1994:260-1.
Forbes CD, Jackson WF, eds. Endocrine, metabolic and nutritional. Color Atlas and Text of Clinical Medicine. 2nd ed. Barcelona, Spain: Times Mirror International / Mosby; 1997:349.
Gocmen A, Peters HA, Cripps DJ, Bryan GT, Morris CR. Hexachlorobenzene episode in Turkey. Biomed Environ Sci. Mar 1989;2(1):36-43. [Medline].
Poblete-Gutierrez P, Badeloe S, Wiederholt T, Merk HF, Frank J. Dual porphyrias revisited. Exp Dermatol. Sep 2006;15(9):685-91. [Medline]. [Full Text].
Canavese C, Gabrielli D, Guida C, Cappellini MD. [Nephrologists and porphyrias] [Italian]. G Ital Nefrol. Jul-Aug 2002;19(4):393-412. [Medline].
Doss MO, Stauch T, Gross U, et al. The third case of Doss porphyria (delta-amino-levulinic acid dehydratase deficiency) in Germany. J Inherit Metab Dis. 2004;27(4):529-36. [Medline].
Hedger RW, Wehrmacher WH, French AV. Porphyria syndrome associated with diabetic nephrosclerosis and erythropoietin. Compr Ther. 2006;32(3):163-71. [Medline].
Rememberâ?¦..Research is the key to your cure!
Series: Porphyria life my Journey ~ Part 1
Friday - September 27, 2013 @ 17:15:56
Choices, decisions, what medications should I take, why do I have to see the Doctor for that matter what kind of Doctor do I need to see and why? This porphyria disease has me really worried What do I say to to Doctor how do I describe what I feel. Do I share the emotional side of it the physical side what it does to me, I know I can do this but right now, I'm not feeling good at all. I have to face a new staff and new doctor, will they listen? will they care? Have they ever heard of this disease? Will they understand and listen to me. I'm so scared, nervous and sick. Where do I begin?????????? Has this ever happened to you? I really would like your input I will be writing a short series weekly so that we can discuss things on this blogs. Many of these questions we have all faced and the worries that go along with it. So please take some time to really think about this stage maybe it was so long ago, maybe your new with this, maybe your waiting and don't know if you have it. I will be sharing my personal struggles, feelings and journey so far. So please take some time to think, ask questions and contribute to this because we succeed as a group not alone. Please share your type, experience in this part above next week- How to pick the right doctor to care for me and why
Amy Chapman 39 and I have AIP
Rememberâ?¦..Research is the key to your cure!
Questions from Facebook and U.S. Porphyria Labs
Friday - September 27, 2013 @ 17:12:59
Many of you have also FB and ask where to send your labs to here is some additional Information for you and your healthcare team.
U.S. Porphyria labs
There are only a few laboratories in the United States that can perform the complex analysis to diagnose Porphyria. The laboratories listed with a ** are overseen by a Porphyria expert who can consult with your physician about your test results. It is always best to have your doctor's office call the laboratory before sending samples to verify collection and shipping instructions.
ARUP Laboratories** University of Utah 500 Chipeta Way Salt Lake City, UT 84108 (801) 583-2787
Fairview University Diagnostic Laboratories University Campus, Mayo Bldg., Room D-293 420 Delaware Street SE (UH-198) Minneapolis, MN 55455 (612)-273-7838 Please note: This lab does urine tests on site; blood and stool samples are sent out to the University of Texas, Galveston Porphyria Laboratory for testing and interpretation.
Mount Sinai Medical Center** Department of Human Genetics Dana Doheny, MS, CGC, Genetic Counselor Porphyria DNA Testing Laboratory Department of Human Genetics & Genomic Sciences Mount Sinai School of Medicine 1425 Madison Avenue, Room 14-74, Box 1498 New York, NY 10029-6574 Tel: (212) 659-6779 Email: porphyria@mssm.edu DNA testing for six porphyrias: AIP, HCP, VP, f-PCT, EPP, CEP
Quest Diagnostics 33608 Ortega Highway San Juan Capistrano, CA 92690 (800) 642-4657
AT PRESENT LABCORP & QUEST ARE NOT RECOMMENDED FOR EPP TESTING
Mayo Medical LaboratoriesTel: (800) 533-1710 or (507) 266-2888 Fax: (507) 266-2888 Please note: The physician or hospital ordering the tests should phone ahead to the laboratory before ordering tests or shipping samples. Telephone consultation is provided to health care professionals only. Direct patient consultation is not provided over the telephone.
Rememberâ?¦..Research is the key to your cure!
Back by Popular Demand! Directions For Collecting A 24-Hour Urine Sample
Friday - September 27, 2013 @ 13:46:37
Directions For Collecting A 24-Hour Urine Sample
Many, many of you have been private messaging me about the proper way to collect for your 24 hour urine sample please use this handout for the labs and with your Doctor.
Many members have asked about the proper way to collect a 24-hour urine. Here are the directions from one Porphyria laboratory. You might want to compare these directions with those from your own laboratory.
Please use a dark plastic jug for collecting the urine. The urine should be protected from light during collection and during shipping. Add 5 grams of sodium carbonate, a powder that will readily dissolve in the urine, to the jug. This adjusts the acidity of the urine and helps preserve the substances the lab will be measuring. It is not toxic or irritating.
A 24-hour urine collection must be started at a specific time and then ended at the same time the next day. You can choose any time that is convenient for you to start the collection. But you must also be sure that you can end the urine collection at the same time the next day.
Record the time that you have chosen to start the collection. You need to start the urine collection with an empty bladder. Therefore, at exactly this time, empty your bladder and discard the urine. In other words, when you start the urine collection, you should empty your bladder and not add that urine to the jug.
From that time on, add any urine that you pass to the jug. You do not need to record the time each time you urinate.
During the collection, store the urine jug tightly capped in a refrigerator or place it in an ice chest.
Exactly 24 hours after you start the urine collection, you should end the urine collection by emptying your bladder into the jug for the last time.
The University of Texas Medical Branch Porphyria Lab primer on testing for Porphyria is available here: www.utmb.edu/pmch/porphyria/
Rememberâ?¦..Research is the key to your cure!
A Poem~ If you could live in my body
Tuesday - September 24, 2013 @ 15:48:17
If you could live in my body
If you could live in my body, just for a day, maybe you wouldnt think that I feel okay. You might understand what its like to be tired by just trying to live, just doing whats required. If you could live in my body you might begin to see, that a simple drug wont set me free. If you could live in my skin youd learn to understand that its not in my head, nor was it planned. I dont want your pity or to make you resent. But I dont need to apologize, or have your consent. I am sick and Im tired every single day, and it wont help to ignore it. So listen when I say: it helps when I relax with a friend and some tea. You cant understand but please, believe me.
Submitted by Beth Turner
Rememberâ?¦..Research is the key to your cure!
Welcome notes.
Tuesday - September 24, 2013 @ 15:40:07
Welcome all new friends and family to the American Porphyria FB groups. We so happy that you can join us. Please take some time to take a look at the following sites to help you become more familiar with Porphyria by visiting porphyriafoundation.com. You can also join the Purple Light Blog to receive stories, tips and information on how others cope with porphyria @http://porphyriafoundation.blogspot.com/
You can also call the APF@ 1-866-APF-3635 or their email is porphyrus@aol.com Rememberâ?¦..Research is the key to your cure!
The single best way to protect against the flu is to get vaccinated each year.
Flu Vaccination
Why should people get vaccinated against the flu?
Influenza is a serious disease that can lead to hospitalization and sometimes even death. Every flu season is different, and influenza infection can affect people differently. Even healthy people can get very sick from the flu and spread it to others. Over a period of 31 seasons between 1976 and 2007, estimates of flu-associated deaths in the United States range from a low of about 3,000 to a high of about 49,000 people. During a regular flu season, about 90 percent of deaths occur in people 65 years and older. The seasonal flu season in the United States can begin as early as October and last as late as May.
During this time, flu viruses are circulating in the population. An annual seasonal flu vaccine (either the flu shot or the nasal-spray flu vaccine) is the best way to reduce the chances that you will get seasonal flu and spread it to others. When more people get vaccinated against the flu, less flu can spread through that community.
How do flu vaccines work?
Flu vaccines (the flu shot and the nasal-spray flu vaccine (LAIV)) cause antibodies to develop in the body about two weeks after vaccination. These antibodies provide protection against infection with the viruses that are in the vaccine.
The seasonal flu vaccine protects against the influenza viruses that research indicates will be most common during the upcoming season. Traditional flu vaccines (called trivalent vaccines) are made to protect against three flu viruses; an influenza A (H1N1) virus, an influenza A (H3N2) virus, and an influenza B virus. In addition, this season, there are flu vaccines made to protect against four flu viruses (called quadrivalent vaccines). These vaccines protect against the same viruses as the trivalent vaccine as well as an additional B virus.
Traditional flu vaccines made to protect against three different flu viruses (called trivalent vaccines) are available. In addition, this season flu vaccines made to protect against four different flu viruses (called quadrivalent vaccines) also are available.
The trivalent flu vaccine protects against two influenza A viruses and an influenza B virus. The following trivalent flu vaccines are available:
Standard dose trivalent shots that are manufactured using virus grown in eggs. These are approved for people ages 6 months and older. There are different brands of this type of vaccine, and each is approved for different ages. However, there is a brand that is approved for children as young as 6 months old and up. Seasonal Flu Shot: Questions and Answers
The quadrivalent flu vaccine will protect against two influenza A viruses and two influenza B viruses. The following quadrivalent flu vaccines will be available:
(*Healthy indicates persons who do not have an underlying medical condition that predisposes them to influenza complications.)
CDC does not recommend one flu vaccine over the other. The important thing is to get a flu vaccine every year.
Are any of the available flu vaccines recommended over others?
No. CDC does not recommend one flu vaccine over another. This includes deciding between trivalent or quadrivalent vaccine or between injection (the flu shot) or nasal spray vaccine. The important thing is to get a flu vaccine every year. Talk to your doctor or nurse about the best options for you and your loved ones.
People who have ever had a severe allergic reaction to eggs, or who have a severe allergy to any part of this vaccine, may be advised not to get vaccinated. People who have had a mild reaction to eggthat is, one which only involved hivesmay receive the flu shot with additional precautions. Make sure your healthcare provider knows about any allergic reactions. Most, but not all, types of flu vaccine contain small amount of egg.
Flu vaccination should begin soon after vaccine becomes available, ideally by October. However, as long as flu viruses are circulating, vaccination should continue to be offered throughout the flu season, even in January or later. While seasonal influenza outbreaks can happen as early as October, most of the time influenza activity peaks in January or later. Since it takes about two weeks after vaccination for antibodies to develop in the body that protect against influenza virus infection, it is best that people get vaccinated so they are protected before influenza begins spreading in their community.
Flu vaccine is produced by private manufacturers, so availability depends on when production is completed. Shipments began in late July and August and will continue throughout September and October until all vaccine is distributed.
Flu vaccines are offered in many locations, including doctors offices, clinics, health departments, pharmacies and college health centers, as well as by many employers, and even in some schools.
Even if you dont have a regular doctor or nurse, you can get a flu vaccine somewhere else, like a health department, pharmacy, urgent care clinic, and often your school, college health center, or work.
The following Vaccine Locator is a useful tool for finding vaccine in your area.
Why do I need a flu vaccine every year?
A flu vaccine is needed every year because flu viruses are constantly changing. Its not unusual for new flu viruses to appear each year. The flu vaccine is updated annually to keep up with the flu viruses as they change.
Also, multiple studies conducted over different seasons and across vaccine types and influenza virus subtypes have shown that the bodys immunity to influenza viruses (acquired either through natural infection or vaccination) declines over time.
Does flu vaccine work right away?
No. It takes about two weeks after vaccination for antibodies to develop in the body and provide protection against influenza virus infection. Thats why its better to get vaccinated early in the fall, before the flu season really gets under way.
Can I get seasonal flu even though I got a flu vaccine this year?
Yes. There is still a possibility you could get the flu even if you got vaccinated. The ability of flu vaccine to protect a person depends on various factors, including the age and health status of the person being vaccinated, and also the similarity or match between the viruses used to make the vaccine and those circulating in the community. If the viruses in the vaccine and the influenza viruses circulating in the community are closely matched, vaccine effectiveness is higher. If they are not closely matched, vaccine effectiveness can be reduced. However, its important to remember that even when the viruses are not closely matched, the vaccine can still protect many people and prevent flu-related complications. Such protection is possible because antibodies made in response to the vaccine can provide some protection (called cross-protection) against different but related influenza viruses. For more information about vaccine effectiveness, visitHow Well Does the Seasonal Flu Vaccine Work?
Will this season's vaccine be a good match for circulating viruses?
It's not possible to predict with certainty which flu viruses will predominate during a given season. Over the course of a flu season, CDC studies samples of flu viruses circulating during that season to evaluate how close a match there is between viruses used to make the vaccine and circulating viruses. Data are published in the weekly FluView. In addition, CDC conducts studies each year to determine how well the vaccine protects against illness during that season. The results of these studies are typically published following the conclusion of the flu season and take into consideration all of the data collected during the season. Interim studies also may be conducted that provide preliminary estimates of the vaccines benefits that season using data available at that time. For more information, see Vaccine Effectiveness How Well Does the Flu Vaccine Work?
Flu viruses are constantly changing (called antigenic drift) they can change from one season to the next or they can even change within the course of one flu season. Experts must pick which viruses to include in the vaccine many months in advance in order for vaccine to be produced and delivered on time. (For more information about the vaccine virus selection process visit Selecting the Viruses in the Influenza (Flu) Vaccine.) Because of these factors, there is always the possibility of a less than optimal match between circulating viruses and the viruses in the vaccine.
Can the vaccine provide protection even if the vaccine is not a "good" match?
Yes, antibodies made in response to vaccination with one flu virus can sometimes provide protection against different but related viruses. A less than ideal match may result in reduced vaccine effectiveness against the virus that is different from what is in the vaccine, but it can still provide some protection against influenza illness.
In addition, even when there is a less than ideal match or lower effectiveness against one virus, it's important to remember that the flu vaccine may protect against the other flu viruses included in the vaccine.
For these reasons, even during seasons when there is a less than ideal match, CDC continues to recommend flu vaccination. This is particularly important for people at high risk for serious flu complications, and their close contacts.
No, a flu vaccine cannot cause flu illness. Flu vaccines that are administered with a needle are currently made in two ways: the vaccine is made either with a) flu vaccine viruses that have been inactivated and are therefore not infectious, or b) with no flu vaccine viruses at all (which is the case for recombinant influenza vaccine). The nasal spray flu vaccine does contain live viruses. However, the viruses are attenuated (weakened), and therefore cannot cause flu illness. The weakened viruses are cold-adapted, which means they are designed to only cause infection at the cooler temperatures found within the nose. The viruses cannot infect the lungs or other areas where warmer temperatures exist.
Different side effects can be associated with the flu shot and nasal spray flu vaccines. These side effects are mild and short-lasting, especially when compared to symptoms of influenza infection.
The flu shot: The viruses in the flu shot are killed (inactivated), so you cannot get the flu from a flu shot. Some minor side effects that could occur are:
Soreness, redness, or swelling where the shot was given
Fever (low grade)
Aches
The nasal spray: The viruses in the nasal spray vaccine are weakened and do not cause severe symptoms often associated with influenza illness. In children, side effects from the nasal spray can include:
Runny nose
Wheezing
Headache
Vomiting
Muscle aches
Fever
In adults, side effects from the nasal spray vaccine can include
Runny nose
Headache
Sore throat
Cough
If these problems occur, they begin soon after vaccination and are mild and short-lived. Almost all people who receive influenza vaccine have no serious problems from it. However, on rare occasions, flu vaccination can cause serious problems, such as severe allergic reactions. People who think that they have been injured by the flu shot can file a claim for compensation from theNational Vaccine Injury Compensation Program (VICP).
How much vaccine will be available during 2013-2014?
Manufacturers have projected that they will produce between 135 million and 139 million doses of influenza vaccine for use in the United States during the 2013-2014 influenza season. An estimated 30 million to 32 million of these doses will be quadrivalent flu vaccine. The rest will be trivalent flu vaccine.
Where can I find information about vaccine supply?
Why do manufacturers and distributors take a phased approach to vaccine distribution?
Influenza vaccine production begins as early as 6-9 months before the beginning of vaccine distribution. Even with this early start, it isnt possible to complete the entire production and distribution process prior to flu season, particularly given the limited number of influenza vaccine manufacturing plants in the United States and the large number of doses that are produced each year. Instead, influenza vaccine distribution takes place in a phased fashion over a number of months. It begins in late summer for some manufacturers and vaccine products and usually completes near the end of November or early in December. This system can leave doctors and other vaccine providers with uncertainty about when they can expect to receive their full order of vaccine and can make it difficult for them to plan their vaccination activities. Manufacturers and distributors try to get some vaccine to as many providers as possible as early as possible so that they can begin vaccinating their patients.
What role does the Department of Health and Human Services play in the supply and distribution of the seasonal influenza vaccine?
Influenza vaccine production and distribution are primarily private sector endeavors. The Department of Health and Human Services and CDC do not have the authority to control influenza vaccine distribution nor the resources to manage such an effort. However, the Department has made significant efforts to enhance production capacity of seasonal influenza vaccines, including supporting manufacturers as they invest in processes to stabilize and increase their production capacity.
Tom Collier and his brother both suffered the symptoms of Erythropoietic Protoporphyria nearly all their lives, but until recently they had no explanation for their photosensitivity. Diagnosis finally came when Tom was 64 years old, after a lifetime searching for answers.
As far back as he can remember, Toms problems in the sun started when he was three years old. He remembers running around screaming after being in the sun, and having a horrible stinging, burning pain all over his hands, arms and legs. Toms parents took him to a variety of doctors throughout the 1940s and 50s to diagnose his problem, but like many children with EPP he had no visible symptoms at all. He didnt swell up, and he didnt get red, his parents just knew he was suffering from terrible pain when he went out of doors.
Tom finally heard of porphyria when his brother caught mention of the disease a little more than five years ago and thought the description matched both of their symptoms. Tom started hitting websites and decided that EPP fit the bill for the problems hed had all his life. He says: nothing else came close. Looking for a doctor who could help him, he found Dr. Micheline Mathews-Roth, a dermatologist and EPP expert in Massachusetts, and Dr. Joseph Bloomer, a hepatologist and EPP liver expert in Alabama. Both doctors have studied porphyria both in patients and in the laboratory for more than 30 years and have served on the APF Scientific Advisory Board since its inception.
Dr. Bloomer ordered lab tests and sent them to the porphyria center at the University of Texas Medical Branch in Galveston, where Dr. Andersons lab quickly made the diagnosis of EPP. Shortly afterwards Tom called Dr. Roth in Massachusetts and spoke with her at length. He had the FEP test (one of several recommended annually for people with EPP) and now has a general practitioner who has two other patients with porphyria.
A lifetimes worth of severe sensitivity to the sun had already taught Tom to be careful, so by the time he was diagnosed he was already used to covering up outside, and not spending a lot of time out of doors in the daylight hours. He says when he first sets foot outdoors the sun feels warm on his skin, just like it does for anybody else. But before long his skin becomes just a little bit uncomfortable, and thats his signal that its time to get indoors right away. After the discomfort comes the prickling, stinging, burning pain that is familiar to those with EPP.
Stepping into the shade when he is unavoidably out of doors is helpful to Tom, but he does get EPP symptoms from indirect light as well and unfortunately his symptoms are triggered more quickly on exposure to light than they once were. Indoors, he feels the sting of fluorescent bulbs (like the kind used in most stores and hospitals), and incandescent bulbs bother him somewhat too.
These days Tom is thinking about having photoprotective window films installed on the glass in his home. When hes out driving, Tom wears long-sleeved shirts and gloves at all times.
It is very easy for porphyria patients, or those with any rare disease, to become impatient with the pace of medicine and the lack of a cure. But keep in mind how far weve come in the past 70 years: from a little boy who screamed in pain and whose parents could find no answers, to a name for the disease, a clear genetic marker for it, and a straightforward diagnostic procedure for ferreting it out. Porphyria patients today owe a tremendous debt not only to the doctors who worked with little recognition and no reward to discover the biological secrets of the disease, but to patients like Tom as well, whose experience helped doctors learn, to all of our benefit.
Rememberâ?¦..Research is the key to your cure!
What is HEP?
Friday - September 13, 2013 @ 10:30:01
Hepatoerythropoietic Porphyria (HEP)
This very rare type of Porphyria is also due to a deficiency of uroporphyrinogen decarboxylase (UROD). The enzyme deficiency is inherited as an autosomal recessive trait. The manifestations of HEP resemble CEP, with symptoms of skin blistering usually beginning in infancy. Porphyrins are increased in bone marrow and red blood cells, in contrast to PCT, as well as liver, plasma, urine and feces.
Rememberâ?¦..Research is the key to your cure!
Need more Z Z Z's?
Wednesday - September 11, 2013 @ 10:30:01
Depression and Sleep: Getting the Right Amount
Lack of sleep can upset your biologic clock and make your depression worse. At the same time, depression can influence your sleeping habits.
A change in your sleep habits is one of the most common effects ofdepression. Lack of sleep can start before depression, be a symptom of depression, and make depression worse.
"Depression and sleep are closely related," says Prashant Gajwani, MD, associate professor and vice chairman of clinical affairs in the department of psychiatry and behavioral sciences at the University of Texas Medical School in Houston. "Depression is a brain illness, and it affects many types of brain functions, including the sleep-wake cycle. Once this biologic clock has been disturbed, it can make sleep even more irregular and that adds to the depression. It can become a vicious cycle for many people."
Effects of Depression on Sleep
People with depression commonly experience disturbed sleep patterns, but the way depression affects sleep varies widely.
"Difficulty getting enough sleep is a major symptom for most people with depression, but for about 10 to 20 percent of people, the effects of depression result in sleeping too much," says Dr. Gajwani. Depression commonly causes:
Difficulty falling asleep
Difficulty staying asleep
Waking up early in the morning
Oversleeping
Sleeping during the day
Poor quality of sleep
Waking up feeling tired
Effects of Sleep on Depression
The amount of restful sleep you are getting can affect your emotional health. "Lack of sleep for a long enough time can cause depression," says Gajwani. Although it is unlikely that lack of sleep alone is responsible for most cases of depression, it may contribute to depression in some people. The fact that many people who have sleep problems develop depression may indicate that sleep disorders and depression have similar causes or risk factors. Links between depression and sleep have been found in many studies, for example:
Research shows that people with insomnia have a 10-fold higher risk of developing depression.
Other types of sleep-related disorders, like obstructive sleep apnea and restless leg syndrome, are associated with high rates of depression. For people with obstructive sleep apnea, depression often improves with apnea treatment.
Research shows that children with depression who experience a lack of sleep or who sleep too much are more likely to have longer and more severe episodes of depression.
Experts suspect that chronic lack of sleep caused by physical illness is one reason older people have higher rates of depression.
Tips for a Good Night's Sleep
If youre having a hard time sleeping at night or you are sleeping away too much of the day, following some healthy sleep habits may help. To start, set a bedtime schedule. "It is very important for people with a history of depression to keep regular hours of sleep, says Gajwani. You should go to bed about the same time and get up about the same time, and use your bedroom only for sleep or sex." Here are some other tips to sleep by:
Exercise. "Make sure to get regular exercise and spend some time outdoors in the sunlight every day. This is a good way to set your biologic clock, and it helps maintain a regular sleep-wake cycle," says Gajwani.
Skip the nap. Avoid afternoon naps, which can lead to nighttime insomnia.
Limit caffeine and alcohol, especially later in the day.Caffeine is a stimulant and can keep you wide awake, while alcohol can disrupt sleep quality. "Alcohol before bedtime will interfere with sleep, warns Gajwani. It may help you fall asleep, but you are less likely to sleep through the night."
Get up if you cant sleep. "Don't waste time lying in bed looking at your clock," says Gajwani. If you find yourself lying awake, the best thing is to get up and do something relaxing until you feel tired.
Shut off the TV. "Avoid watching television late at night. Most shows in the evening are too stimulating and do not promote good sleep, says Gajwani. It's better to read a book or do a relaxing activity in the hours before bed."
Practice good sleep hygiene. This includes using your bedroom primarily for sleeping and sticking to a regular sleep schedule. Avoid distractions in your bedroom, like phones, computers, too much light, and too much noise. Make sure your bed is comfortable and that the room temperature is comfortable for sleeping.
Changes in sleep patterns can be an effect of depression or an early warning sign of it. Let your doctor know if you are not able to sleep or if you are sleeping too much. "Over-the-counter sleep aids are not a good solution for people with depression and sleep problems, says Gajwani. Practice good sleep hygiene, get regular exercise, and work with your doctor or therapist to get your depression under control." Taking care of yourself, including getting the right amount of restful sleep, can help you manage your depression.
Sweet dreams everyone!
Rememberâ?¦..Research is the key to your cure!
American Porphyria Foundation Media News
Tuesday - September 10, 2013 @ 10:30:01
Even for some of the best minds in medicine, porphyria can be puzzlement. When porphyria is unrecognized, patients are often given medications that worsen their condition, undergo multiple unnecessary and dangerous surgeries, or suffer permanent skin damage, severe liver disease or other complications that could be avoided if the disease were better recognized.
Porphyria is known as "the little imitator," because it mimics so many more common conditions. Acute porphyria has been called the "Tic-tac-toe disease," because before the advanced imaging technologies (C/T, MRI, ultrasound) we have today were developed, doctors would perform multiple surgeries in search of the source of a patients abdominal pain, leaving scars in the shape of a Tic-tac-toe game.
Different types of porphyria (and its misdiagnoses) have been featured on Discovery Health's Mystery Diagnosis, and on dramas like House, CSI, and ER. Patient stories have been covered in publications ranging from Ladies' Home Journal to online sports news outlets. There are works of popular fiction and non-fiction about porphyria, notably Isabel Allende's memoir, Paula, written while the authors daughter lay in a coma brought on by an acute attack.
The APF welcomes media attention to these fascinating and troubling diseases. If you are a member of the media, we hope you will use the information you find here in your stories, and we ask that you credit the American Porphyria Foundation as your source. We encourage you to share our website address, www.porphyriafoundation.com, and our toll-free telephone number, 1-866-APF-3635, with your audience as well.
Please call our office for additional information.
Porphyria in the Media
"Perplexing Pain," a mysterious case story of acute porphyria from the New York Times, Sunday Magazine November 1, 2009. (Page 1, Page 2)
"Rare genetic disorder doesn't slow down boys," two brothers in a small Texas town deal with erythropoietic protoporphyria (EPP) from the Vernon Daily Record April 9, 2010. (1, 2,3)
"The Mystery Illness" of Congenital Erythropoietic Protoporphyria (CEP) on Dr. Dean Edell's Medical Journal, ABC-TV 1986. (on genebennett.net)
Please contact us for a complete listing of print, radio and television features. 1-866-apf-3635
Rememberâ?¦..Research is the key to your cure!
Fundraiser or Special Event Volunteer
Monday - September 9, 2013 @ 16:06:43
Fundraiser or Special Event Volunteer
It's about that time when the cooler weather hits and we do some out door races, running, skiing or out door fun activity have you considered holding a special event and awareness
for the American Porphyria Foundation? Let's get creative, involved and work together!
Let's have some FUN!
Thanks to the efforts of our fund-raising volunteers, revenue generated through special events fundraising helps the APF link members through the In Touch network, fund research, and educate physicians, patients and the general public about porphyria. There are many creative ways to raise money, and we can guide you in designing a fundraiser that will be easy for you to run. Some people enjoy hosting community events like a run or a raffle. Others prefer neighborhood events like a spaghetti dinner or bake sale.
Many of our members have written a letter to their family, friends, co-workers or religious community to let them know how the APF has helped them and asking recipients to give to the APF. Doing this will help educate others about a condition that has deeply affected your life, and help other porphyria patients at the same time.
Many families have had success asking people to donate in honor of a birthday, or in memory or honor of someone special to them.
Be sure to let people you write to know: 1) What you are asking them to do and why; 2) What porphyria has meant to you; 3) How the APF has affected your life; and 4) How to donate.
Before you begin planning a fundraiser, please contact us at the APF office (866-APF-3635 or 713-266-9617). Remember, we are here to help you meet your fundraising goals. We can help you brainstorm, provide suggestions and put you in touch with others who have organized similar events. Thank you for your help, and happy fundraising!
Rememberâ?¦..Research is the key to your cure!
The Bogus Connection between "MCS" and Porphyria Stephen Barrett, M.D.
Friday - September 6, 2013 @ 10:30:03
The Bogus Connection between "MCS" and Porphyria
Stephen Barrett, M.D.
Porphyria is a well-defined group of disorders caused by abnormalities in the chemical steps that lead to heme production. Heme, a molecule needed by all of the body's organs, is found mostly in the blood, bone marrow, and liver. Heme is a component of hemoglobin, the molecule that carries oxygen in the blood [1]. The signs and symptoms of porphyria vary among the types. Some types (called cutaneous porphyrias) cause the skin to become overly sensitive to sunlight. Exposed skin may develop redness, blistering, infections, scarring, changes in pigmentation, and increased hair growth. Other types of porphyria (acute porphyrias) mostly affect the nervous system. Appearing quickly and lasting from days to weeks, acute signs and symptoms include abdominal pain, vomiting, constipation, and diarrhea. During an attack, a person may also experience muscle weakness, seizures, fever, loss of sensation, and mental changes such as anxiety and hallucinations. Two forms of porphyria have a combination of acute symptoms and symptoms that affect the skin [1]. Most forms of porphyria are inherited. In contrast, "multiple chemical sensitivity" ("MCS") is a medically disputed term used to describe people with multiple troubling symptoms they attribute to environmental factors. Many such people are seeking special accommodations, applying for disability benefits, and filing lawsuits claiming that exposure to common foods and chemicals has made them ill. Their efforts are supported by a small network of physicians who use questionable diagnostic and treatment methods. Practitioners who promote MCS as a diagnosis claim that it is caused by extremely low levels of chemical substances found in the environment. However, no scientific tests have ever been able to detect an organic basis for the diagnosis, and no major medical organization recognizes MCS as a clinical disease. Instead of testing their claims with well-designed research, its advocates promote them through publications, talk shows, support groups, lawsuits, and political maneuvering [2].
Shifting Claims
In the 1990s, partly in response to the fact that courts were not recognizing MCS as a disease, many proponent doctors began inappropriately diagnosing disorders of porphyrin metabolism in large percentages of their patients [3]. Although the porphyrias are rare, these doctors claim that many MCS patients have porphyrin abnormalities and that the same environmental substances can trigger both conditions [4]. Their strategy was laid bare in a 1996 article in Our Toxic Times which said that diagnosing one of the porphyrias was advantageous because they have a recognized diagnostic code and doctors who dont know about MCS or dont believe in it do believe in porphyria. [5] Another issue of the newsletter contained a porphyria symptom check list of about 90 possible symptoms. [6] Porphyrias do not have that many symptoms. Expert reviewers have concluded that the proposed relationships between MCS and porphyrin disorders should be considered speculative and unestablished and do not justify using any measures that are appropriate for treating porphyrias [7]. In 1995, the Washington State Department of Labor and Industries and the Washington State Medical Association issued an authoritative guide to diagnosing porphyrin disorders [8].
Flawed Laboratory Testing
Most of the purported association of porphyria with MCS is based on results obtained with the urinary coproporphyrin assay, a laboratory test performed by the Mayo Clinic. However, the test has never been validated. Although "MCS" patients reportedly showed modest increases in urinary coproporphyrin excretion, this is a common finding found in many people without symptoms and also in patients with diverse other conditions such as diabetes mellitus, heavy alcohol use, liver disease, and many kinds of anemia. In 1997, two porphyria experts at the University of Massachusetts Medical Center noted these facts and warned that the test was not reliable, had not been validated, and should not be used [9]. In 1999, two Mayo researchers concluded that 56 out of 64 of the enzyme tests performed by the Mayo laboratory should not have been ordered and that there was "substantial overordering" of other tests and "inadequate physician knowledge about the interpretation of test results in the evaluation of acute porphyria." [10] Their report did not reveal the fact that most of the inappropriate enzyme tests were ordered by William Morton, M.D. of Oregon Health Sciences University, who was the MCS-porphyria connection's leading advocate.
Court and Regulatory Actions
I know of three cases in which judges gave no credibility to a porphyrin-MCS connection. In 1991, a trial court ruled that plaintiff's immune assays, including calla and porphyrin antibody testing, performed by Dr. Bertram Carnow, were inadmissible because plaintiff failed to prove that the testing was "acceptable to at least a substantial minority of the relevant scientific community." [11] In 2001, an administrative law judge ruled against a claimant who sought compensation for alleged work-related porphyrin deficiency and relied on testimony of Dr. Morton. According to a case summary I found on the Internet:
The [Administrative Law Judge] rejected Dr. Mortons opinion because it was clear that Dr. Mortons opinion was not based upon the same level of intellectual rigor that characterizes the practice of experts in this field of medicine. Dr. Morton was outside of the medical mainstream and his analysis was non-scientific since his description of the disease and environmental causes was so broad as to be meaningless. He also had no scientific basis for rejecting known and accepted testing techniques which were objective, reproducible, and reliable in terms of locating levels of enzyme residue that would be created by this particular disease [12].
In 2004, the Oregon courts ruled against a woman in a similar case, which the appeals court summarized this way:
Throughout 1996 and 1997, after leaving her employment with Lane County, petitioner continued to see her physicians for complaints of chemical reactivity. In May 1997, Dr. Morton, a specialist in occupational medicine, diagnosed petitioner as having "active porphyrin metabolic dysfunction" (i.e., porphyria). He explained that people "with porphyria traits are abnormally susceptible to porphyrogenic substances," such as the fumes from certain types of chemicals and substances. He further explained that, "Once activated, porphyria symptoms do not always stop when the initiating exposure stops." In connection with a workers' compensation claim that petitioner filed with Lane County, petitioner was also examined by Dr. Burton, a specialist in medical toxicology and occupational medicine. In Burton's opinion, petitioner's history and symptoms were not consistent with a diagnosis of porphyria, and petitioner does not suffer from that condition. Burton also opined that the diagnosis of MCS given by one of petitioner's treating physicians was not a legitimate medical diagnosis. In Burton's view, physicians use a diagnosis of MCS to explain a variety of nonspecific symptoms otherwise not organically explainable [13]
In 2001, the Oregon Board charged Morton with inappropriately diagnosing "porphyria" with the result that patients received inappropriate treatment from him or other providers [14]. In 2002, rather than facing the charges, Morton agreed to retire his license [15]. Because Morton was by far the leading proponent of the MCS-porphyria connection, his "retirement" and judicial thrashings signaled the end to what Dr. Burton recently dubbed "the porphyria epidemic." [16] Additional Information
Stipulated order. In the matter of William Edwards Morton, MD before the Board of Medical Examiners, State of Oregon, Jan 17, 2002.
Burton B. E-mail message to Dr. Stephen Barrett, Jan 21, 2010.
This article was revised on January 22, 2010.
Rememberâ?¦..Research is the key to your cure!
CME Course is Back by Popular Demand
Thursday - September 5, 2013 @ 10:30:00
CME Course is Back by Popular Demand
Continuing Medical Education (CME)
Physicians are required to have Annual Continuing Medical Education courses. Fortunately, they have the opportunity to take this outstanding CME course about Acute Porphyrias and receive FREE CME credit. Please tell your doctor about this course which was offered last year and has been brought back by demand and is offered at the following link. CME courses require registration but most physicians are already registered.
Herbert L. Bonkovsky, MD; Manisha Balwani, MD, MS; Karl E. Anderson, MD; Brendan Martin McGuire, MD, MS Faculty and Disclosures. CME Released: 01/19/2010; Reviewed and Renewed: 07/08/2013; Valid for credit through 07/08/2014
This activity is intended for hematologists, gastroenterologists, primary care physicians, emergency medicine physicians, obstetricians/gynecologists, and other healthcare professionals who may encounter patients with the acute porphyrias.
The goal of this activity is to provide an informative discussion on some of the major issues associated with acute porphyrias, including recognition, evaluation, treatment, complications, and prevention.
Upon completion of this activity, participants will be able to:
Recognize signs and symptoms of and conduct appropriate testing to promptly and accurately diagnose the acute porphyrias
Evaluate current recommendations and emerging approaches for the management of the acute porphyrias
Discuss complications associated with the acute porphyrias and their treatment
Rememberâ?¦..Research is the key to your cure!
Porphyria Awareness & Fundraising Events!
Wednesday - September 4, 2013 @ 20:42:36
Past and Present Porphyria Awareness &
Fundraising Events.
*Events are listed below with the most recent Event first.*
~ Official APF Porphyria Awareness T-Shirts are Available Now! Read more.
~ Running over obstacles to raise Awareness for Porphyria. Read more.
~ Amy Chapman's Porphyria Awareness and Fundraising Campaign. Read more.
~ Cook Brothers and Family Promote Awareness Week. Read more.
~ Student Alessia Callahan Educates Classmates during National Porphyria Awareness Week. Read more.
~ Monica's Porphyria Awareness Week Event. Read more.
Coming up soon will be a special event that Polly Barton Harvard will share in and she hopes that you will to more details to come.
Remember..Research is the key to your cure!
Finding a Doctor
Wednesday - September 4, 2013 @ 20:39:21
Finding a Doctor
The American Porphyria Foundation promotes comprehensive care necessary for treating individuals with Porphyria. This section of our website offers suggestions for finding a local doctor who can manage your Porphyria, options for having your doctor consult a Porphyria specialist, and information on arranging a visit to a Porphyria clinic.
Because Porphyria is so rare, few physicians have experience treating patients with the disease. Most patients are in fact treated But the APF can help by putting your doctor's office in touch with a Porphyria specialist who can offer guidance on your care.
For those who need a diagnosis, you may be able to obtain a consultation at Porphyria clinic. Call the APF to reach a porphyria expert at a porphyria center. The APF office will also guide you to doctors who are not experts but are knowledgeable about porphyria. You may be asked to send your blood, urine, and stool samples for evaluation in advance of a clinic appointment. Especially if you plan to travel for a consultation, it is a good idea to call ahead and explain that you would like to be evaluated for Porphyria so that you can be sure you have done any necessary testing in advance. If local video conferencing facilities are available, telemedicine consultation with a Porphyria expert is also available.
Regardless of your situation, it is best to establish a good relationship with a doctor in your area. Developing a relationship with a primary care physician takes time and can be frustrating, particularly when you have difficulty finding a doctor who will manage your care. In this section of the website, you will also find Tips for the Doctor's Office that may help.
If you're having trouble finding a local doctor, the following organizations' doctor finder or physician referral services could be helpful. The APF does not recommend or endorse the doctors listed through these sites.
If you would like to read about supporting programs to ensure the quality of specialists in the field of porphyria, please see our Protect Our Future campaign information.
"Remember.Research is the key to your cure!"
2013 International Porphyria Conference Video and Audio are available
Monday - September 2, 2013 @ 20:24:59
2013 International Porphyria Conference Video and Audio are available
Video and Audio of the International Porphyria Conference are available by joining RareConnect.org.
On the video, representatives from patient groups introduce themselves; tell about the organizations in their respective countries and share patient testimonials.
Porphyria Argentina - Estela Y. Ferrari de Frassia
Orphan Europe- Recordati Group-Panhematin- Think beyond the obvious THINK PORPHYRIA
Tuesday - August 27, 2013 @ 20:21:18
Do you think you could have Acute Porphyria? Do you need to see a Physician for testing? If you have questions please call the American Porphyria Foundation for finding assistance with a Doctor @
866-APF-3635 or visit porphyriafoundation.com for additional materials and help.
"Remember.Research is the key to your cure!"
NEW shipment of APF T-shirts are in get yours today!
Monday - August 26, 2013 @ 12:16:02
The new shipment of APF T-shirts are here!
Our hope for the T-shirts is that you all will buy and wear them to help promote and raise questions about Porphyria and to raise funds for the Dr. Packets, pain Management docs, among many other publications we make available at no cost.
Amy Chapman is heading up the T-shirt project. There are also some copies of Porphyria Live for sale. For information on how to order the T-Shirts and/or the Porphyria Live Video see below.
You can order a T-shirt and/or Porphyria Live DVD by sending an email order toporphyriaorders@gmail.com
I must have name, complete address, and phone number. Also include the Quantity of T-shirts and the size for each one. And include the quanity of the Porphyria Live Video.
To accept payment: One of two options I can accept Paypal VISA/MC only I must have full name on the card, account#, exp. date, 3 digit code on back of card CVV-
I will accept money orders and personal checks. You must have name/address/phone # on them. Your information will be kept confidential and never on file, and will be destroyed promptly after each transaction.
They can be mailed to me:
Amy Chapman
10475 Gandy BLVD N. Unit 3417
St. Petersburg FL 33702.
*The APF will not take orders or calls about T-shirts*
Once I receive the order I will ship out your product.
All products will be shipped out Priority mail with tracking. Each person also will receive a receipt with T-shirts.
T-shirts come in the following sizes S, M, L XL, 2xl, 3xl they are 100% cotton, heavy not thin, and very durable. No other sizes.
The price per T-shirts is $19.00/shirt. This covers the shirt, shipping and tracking, and priority mail. International orders: I will have to consult first with the post office for shipping rates.
The price of the Porphyria Live DVD is $10.00 each. Shipping is included in the price.
100% of all funds received will go back to the APF
"Remember.Research is the key to your cure!"
8-2-13 EPP meeting and Afamelanotide/SCENESSE
Friday - August 23, 2013 @ 17:09:55
August 2, 2013 was a memorable day for the APF members, who met at the FDA to explain Erythropoietic Protoporphyria (EPP) and ask that the FDA approve Afamelanotide/SCENESSE forEPP. Most of the attendees had participated in either the Phase II or Phase III clinical trials and were eager to elaborate on their positive experience on the drug. We sincerely thank Florence Rollwagen, Diana Ijames, Mike Kenworthy, Steve Ferry, Pierre Mouledoux, Mike Ferry, and Andrew Turell, who spoke eloquently about EPP and its effect on their lives. Each person presented unique aspects of dealing with EPP, as well as their experience with the treatment. It was poignant to hear how a daily life of pain, isolation and anxiety was changed when they receivrd the implant. Johnathan Turell, and Kristen Wheeden spoke about being parents of a loved one with EPP and shared the family dynamics that occur with the disease.
We also thank Desiree Lyon Howe, who arranged the meeting with the FDA and gave an overview of the APF efforts for the Phase II and Phase III clinical trials, as well as discussed the Porphyria Research Consortium of porphyria experts and their research on Afamelanotide. Our appreciation goes to the co-chairs of the Porphyria Research Consoritum, Drs Robert Desnick and Karl Anderson, who explained the disease and spoke on their research on Afamelanotide and their views on the beneficial effect it had on the research volunteers.
Each of the presentations to the FDA representatives was outstanding. We hope they will assist the FDA in understanding the importance of approving a treatment for EPP, specifically approval of Afamelanotide as soon as possible.
"Remember..Research is the key to your cure!"
Diet Information for All Porphyrias
Wednesday - August 21, 2013 @ 13:24:08
Diet Information for All Porphyrias
Nutritional Advice for Persons with Porphyria
Herbert L. Bonkovsky, MD
Jessy Philip, RD, PhD
Carolinas Health Care System, Charlotte, NC
Department of Medicine, Univ of CT Health Center and Univ of NC School of Medicine
Overview: Good nutrition is important for all of us, including those with porphyria. For the most part, persons with porphyria should follow the sensible and usual dietary advice of the Centers for Disease Control, the US Department of Agriculture, and other responsible and reputable governmental agencies.
Because over-nutrition and obesity are such a great problem in the USA and other western countries, it is important that patients with porphyria do their best to avoid becoming obese or gaining weight beyond their ideal body weights. The acute porphyrias [acute intermittent porphyria, hereditary coproporphyria, variegate porphyria, and ALAD deficiency porphyria] may be made worse by prolonged fasting or severe ['crash'] dieting, because, in these forms of porphyria, glucose and other carbohydrates help to repress the activity of hepatic ALA synthase 1, the first enzyme of the heme synthetic pathway. In these forms of porphyria, uncontrolled up-regulation of ALA synthase 1 in the liver is a necessary component of the metabolic abnormalities that may give rise to acute attacks.
General Advice: There is no special or particular diet required or recommended for persons with porphyria. Rather, the principles of good and sensible nutrition apply. These principles call for a varied and balanced diet, particularly with avoidance of over-nutrition. Consumption of too many calories, in excess of daily needs for calorie and energy consumption, has emerged as one of the greatest public and personal health problems of Americans. The growing problem of obesity is present in much of the world, not just in North America.
Figure 1 shows current general dietary recommendations for Americans, as developed by the Department of Health and Human Services and the Centers for Disease Control. http://health.gov/dietaryguidelines/2010.asp Such advice should be followed by persons with porphyria, as well as those without. The keys are adherence to a varied and balanced diet with balanced, moderate consumption of carbohydrates, protein, and fats. To reduce the risks of cardiovascular diseases, such as atherosclerosis or heart attacks, the fats should include little or no trans-fats and preferably include a substantial proportion as unsaturated fatty acids [such as olive oil, safflower oil], rather than saturated fatty acids [such as animal fat]. The protein may be in the form of animal or vegetable protein. The carbohydrates should preferably not include large amounts of refined sugars or high fructose corn syrup, although oral or intravenous carbohydrate in the form of dextrose may be prescribed for therapy of acute attacks of porphyria. However, day in and day out, even persons with one of the acute porphyrias should not be consuming large amounts of dextrose (sugar) or fructose.
Nutritional Advice for Persons with Acute Porphyria. The acute or inducible porphyrias include acute intermittent porphyria (AIP), hereditary coproporphyria (HCP), variegate porphyria (VP), and porphyria due to severe deficiency of ALA dehydratase (ALADP). Most persons that have one of these forms of porphyria, all of which are due to inherited deficiencies in one of the enzymes of heme biosynthesis, have no symptoms or signs of porphyria most of the time. They may, however, occasionally develop acute attacks, usually characterized by severe bouts of abdominal pain with increases in blood pressure and pulse rate and with severe constipation. Sometimes, the pain may be in the chest, back or extremities instead of, or in addition to, the abdomen [belly]. Such attacks are characterized by a marked up-regulation of an enzyme in the liver called delta-aminolevulinic acid synthase 1 (ALAS1). This up-regulation leads to a marked over production and urinary over-excretion of delta-aminolevulinic acid (ALA) and porphobilinogen (PBG), which are the biochemical hallmarks of acute porphyric attacks.
The treatment of such acute attacks is focused on decreasing the up-regulation of hepatic ALAS1. This is done by the administration of sugar [dextrose] and by the administration of heme, which must be given intravenously. During acute attacks, patients often have nausea and vomiting, as well as disturbances of normal gastrointestinal function, so that it is necessary for the dextrose to be administered intravenously, as well. If the attacks are less severe, however, patients may be able to take in dextrose orally, such as by adding sugar to orange juice, by sucking on hard candies, etc. During such acute attacks, the usual therapeutic recommendations by experienced physicians are for the daily intake of dextrose or other metabolizable carbohydrates to be approximately 300 grams per day.
It is also important for persons with one of the acute porphyrias to avoid drugs or other factors that are known to be able to trigger acute attacks. Chief among these are estrogen and especially progesterone. Thus, some menstruating women unfortunately experience monthly symptoms during the middle of their menstrual cycles, around the time of ovulation, when their endogenous production of progesterone is at a peak. Such women may benefit from drugs such as gonadotropin-releasing hormone antagonists [leuprolide] or low doses of oral contraceptives, which interrupt their normal monthly hormonal cycles. Some benefit from receiving prophylactic infusions of Panhematin on a monthly basis, typically administered shortly before the time of the month when they ovulate [mid-menstrual cycle].
A number of drugs and chemicals are capable of up-regulating hepatic ALAS1 and are thus best avoided by persons with acute porphyria. Such drugs include barbiturates, such as phenobarbital, hydantoins such as phenytoin and carbamazepine, sulfonamides such as sulfamethoxazole or sulfisoxazole [and many others]. Another factor that is capable of triggering acute porphyric attacks is excess intake of alcoholic beverages. Thus, persons with acute porphyria should avoid any binge drinking. Good general advice is that men should drink alcohol either not at all or not more than two drinksl per day and women should drink not all or not more than one drink of alcohol per day.
Any acute stress such as an acute illness or severe emotional or psychological stress or exhaustion may also trigger acute porphyric attacks. Therefore, patients with acute porphyria should receive vaccinations to protect them from preventable acute infections, including annual flu shots, Pneumovax [a vaccination that protects against development of pneumonias], vaccinations to protect against diphtheria pertussis and tetanus, with booster shots for tetanus at least every ten years, vaccinations to protect against hepatitis A or hepatitis B infection, and for those who have had chicken pox, the vaccination to protect against development of shingles (Zostrix).
There is no convincing clinical or scientific evidence that any particular foods (with the exception of alcoholic beverages, as described above) are capable of triggering or worsening acute porphyric attacks. There are, however, some foods that have been shown to contain chemical substances that, in large amounts, can up-regulate hepatic ALA synthase 1. Such foods include charcoal-broiled meats, cabbage, and Brussels sprouts. The amounts of such foods that would need to be eaten in order to produce induction of hepatic ALA synthase 1 have not been carefully studied, but are probably far above the amounts that would be eaten as part of reasonable, well balanced diets. None of these foods needs to be avoided completely by persons with acute porphyria, unless they have true allergies to them, which are very uncommon. Moderation in all things is the best course of action. The Appendix lists suggested meal plans for persons with acute porphyria who are of normal weight and with normal daily needs for energy [~30-35 Kcal/kg BW/d].
Dieting in Acute Porphyria. It is important that persons with acute porphyria avoid crash diets with extreme decreases in daily carbohydrate and caloric intakes. However, it is also important that they avoid obesity. If they already are obese, they should gradually lose weight. This should be done with a formal diet plan and under the supervision of an experienced physician and nutritionist.
Sulfur Containing Amino Acids and Essential Amino Acids. Our normal diets contain proteins. In fact, regular and adequate intake of protein is essential to normal growth and health. Proteins are found in both vegetable and animal sources of foods. The building blocks of proteins are called amino acids. Some of these amino acids, such as methionine and cysteine, contain sulfur. Such amino acids are not the same thing as "sulfa drugs". They are not contraindicated for patients with acute porphyria. In fact, methionine is one of the nine essential amino acids: if adequate amounts of these nine amino acids [histidine, isoleucine, leucine, lysine, methionine, phenylalanine, threonine, tryptophan, and valine] are not consumed regularly, deficiencies will develop that can lead to malnutrition and disease. The reason is that humans are unable to make these amino acids and must take them in regularly, in order to achieve and maintain adequate levels to permit their bodies to make the hundreds of thousands of proteins that are essential for good health.
Porphyria Cutanea Tarda [PCT]. The major risk factors for the development of porphyria cutanea tarda are excess alcohol intake, cigarette smoking, increased iron, certain chronic viral infections, especially hepatitis C virus and human immunodeficiency virus, and estrogens. About 20 to 25% of persons with porphyria cutanea tarda (PCT) also have a genetic predisposition in the form of a inherited partial deficiency of an enzyme called uroporphyrinogen decarboxylase. However, such a deficiency in itself is not sufficient to produce symptomatic PCT; other factors are also needed.
The main dietary advice for persons with porphyria cutanea tarda is to avoid all alcohol in any form. In addition, adherence to a low iron diet with avoidance of any medicinal iron and with ingestion of limited amounts of liver or red meat, is recommended, at least until remission of active PCT has been achieved. Remission is achieved by the removal of iron, usually by therapeutic phlebotomy, which is the removal of one unit of blood every week or two. This is continued until an iron reduced state has been achieved. Patients with active PCT typically require the removal of eight to twelve pints of blood, although this number is variable. The progress of iron removal is best followed with serial measurements of serum ferritin. The ideal serum ferritin is 50 to 100 ng per ml. Typically, removal of one pint of blood will lead to a decrease in serum ferritin of about 30 ng per ml. An alternative for the treatment of PCT, especially without acquired or inherited iron overload [hemochromatosis] is the use of low dose-antimalarial drugs, such as chloroquine or hydroxy-chloroquine.
Erythropoietic Protoporphyria [EPP]. In EPP there is excess production of protoporphyrin by developing red blood cells in the bone marrow. This is due usually to an inherited deficiency in an enzyme called ferrochelatase or heme synthase, the final enzyme in the heme synthetic pathway. A less common form of EPP is caused by an increase in activity of the erythroid form of ALA synthase [ALAS2], the first enzyme of the heme synthetic pathway.
Many persons with EPP have a mild degree of anemia with measures of iron that suggest iron deficiency. Some such persons appear to benefit from iron administration, although often, despite taking medicinal iron, they continue to have low levels of serum iron, increases in iron binding capacity, and low levels of serum ferritin, suggesting that they are not absorbing the iron in a normal way. For unknown reasons, a few persons with EPP and evidence of iron deficiency have seemed to worsen with iron administration. Therefore, use of medicinal iron supplements in EPP should be undertaken carefully and with careful monitoring by an experienced physician.
There also have been a few reports that intake of glucose has led to an improvement in EPP. In addition, the use of intravenous heme [which contains iron] has been found to help improve liver damage in persons with EPP.
For the most part, there is no particular special diet recommended for patients with EPP. A varied well balanced diet with avoidance of excess calories and with assurance of adequate intakes of iron and other minerals and vitamins is recommended.
Rare Cutaneous forms of Porphyria. Congenital Erythropoietic Porphyria. CEP is a rare genetic disorder characterized by deficient activity of an enzyme called uroporphyrinogen 3 synthase (also sometimes called uroporphyrinogen co-synthase). It is characterized by severe over-production of uroporphyrin 1, which is manifest at birth and in the neonatal period. There is no particular diet that is indicated or recommended for persons with CEP. The same thing may be said of the rare form of cutaneous porphyria called hepato erythropoietic porphyria, which presents in the new born period, as does CEP, but which is due to severe deficiency of uroporphyrinogen decarboxylase (homozygous or compound heterozygous deficiency).
Advice about Vitamins and Minerals: For mostAmericans who are consuming mixed, well-balanced diets, there is no need for routine use of vitamin or mineral supplements. Persons who consume few dairy products [milk, yogurt, cheese, etc] and older persons, especially women, and those with little exposure to sunlight are prone to develop deficiencies of vitamin D and to have inadequate intake of calcium. Thus, they should have their serum levels of 25-hydroxy vitamin D checked and should seek advice of a well-trained physician or nutritionist regarding supplements of vitamin D and calcium. There is potential harm from the excessive intake of vitamin D or calcium, or of excessive intakes of other fat-soluble vitamins [vitamins A and E]. Thus, moderation in intake is best. There is little harm, but also little likelihood of benefit, in the intake of water-soluble vitamins [vitamins B and C]. Iron may trigger or worsen porphyria cutanea tarda, and it may also increase levels of hepatic ALA synthase 1. Thus, it should not be taken in medicinal form unless there is evidence of iron deficiency. There is little reason for anyone with porphyria [or most without porphyria] to take in supplemental copper, zinc, selenium, chromium, silver, gold, or other metals.
Advice about Herbal Remedies and Dietary Supplements. Herbal remedies and dietary supplements (HDS) have become popular in the USA and in many other parts of the world. In fact, there is widespread irrational enthusiasm for taking such supplements. We recommend against their use because the composition and purity of them are uncertain. They are unregulated by the US Food and Drug Administration, and they have not been shown to be safe and effective. Many of them probably contain chemicals that are capable of up-regulating hepatic ALAS1 and thus of triggering or exacerbating acute porphyria. In addition, they often are adulterated with potentially toxic substances, such as heavy metals.
"Remember..Research is the key to your cure!"
CME Course
Monday - August 19, 2013 @ 16:24:31
Continuing Medical Education (CME)
Physicians are required to have Annual Continuing Medical Education courses. Fortunately, they have the opportunity to take this outstanding CME course about Acute Porphyrias and receive CME credit. Please tell your doctor about this course which was offered last year and has been brought back by demand and is offered at the following link. CME courses require registration but most physicians are already registered.
Herbert L. Bonkovsky, MD; Manisha Balwani, MD, MS; Karl E. Anderson, MD; Brendan Martin McGuire, MD, MS Faculty and Disclosures. CME Released: 01/19/2010; Reviewed and Renewed: 07/08/2013; Valid for credit through 07/08/2014
This activity is intended for hematologists, gastroenterologists, primary care physicians, emergency medicine physicians, obstetricians/gynecologists, and other healthcare professionals who may encounter patients with the acute porphyrias.
The goal of this activity is to provide an informative discussion on some of the major issues associated with acute porphyrias, including recognition, evaluation, treatment, complications, and prevention.
Upon completion of this activity, participants will be able to:
Recognize signs and symptoms of and conduct appropriate testing to promptly and accurately diagnose the acute porphyria
Evaluate current recommendations and emerging approaches for the management of the acute porphyrias
Discuss complications associated with the acute porphyrias and their treatment
"Remember..Research is the key to your cure!"
Protecting Your Job While Coping With a Chronic Illness
Monday - August 19, 2013 @ 16:09:42
Protecting Your Job While Coping With a Chronic Illness
Dawn Villella for The New York Times
Natasha Frechette, diagnosed with multiple sclerosis two years ago, has continued her job at Navigo Research in Brooklyn Park, Minn., with the help of an understanding boss and supportive colleagues.
IT started with an odd sensation in her right hand and a feeling of exhaustion so profound she could hardly get through an hour of work, let alone a full day.
After numerous tests and countless doctors visits, Natasha Frechette, then 27, learned she had multiple sclerosis, a disease that attacks the central nervous system and can cause numbness, blindness and eventualparalysis.
In addition to grappling with the diagnosis, Ms. Frechette was concerned about keeping her job as a data manager for a small research organization in Brooklyn Park, Minn. I didnt want to have to depend on someone to take care of me, she said. "But I know that I could wake up tomorrow and not be able to walk."
Workers with chronic illnesses face chronic uncertainty, forced to worry not only about their health but about their jobs as well. The protections afforded chronically ill workers in the United States are thin and somewhat vague. To protect their health and their jobs, workers must navigate employers policies, which may include short- and long-term disability plans, as well as a patchwork of federal laws and regulations.
A recent study by the Center for Economics and Policy Research, a Washington research organization, found that among 22 rich nations, the United States was the only one that did not guarantee workers paid time off for illness.
Most other countries provide their workers not only with paid sick days, but also time off for cancer treatments, the study found. German citizens, for example, are allowed five sick days and 44 days for cancer treatment, if needed, in addition to vacation days.
Most employers in the United States allow employees to take days off for minor ailments, like the flu or outpatient operations, without docking their pay. And 41 percent offer employees days off nine, on average for illness or other reasons, in addition to vacation days, according to a 2007 survey by Mercer, a benefits consulting business based in New York.
But when an employee has a serious or chronic illness, like diabetes, major depression orlupus, the rules about time off become murky.
Two laws offer workers some relief. The Family and Medical Leave Act allows employees to take up to 12 weeks off each year for medical or family emergencies but without pay. And the Americans With Disabilities Act requires employers to make reasonable adjustments for disabled workers, often in the form of additional time off.
Ms. Frechette explained her condition to her supervisor and said she would need time off for physical and occupational therapy. Her boss readily agreed, and Ms. Frechette, who plans to marry this fall, continues to work full time.
Im careful, she said. "I dont want my disease to be seen as a cop-out.
If you are dealing with an chronic illness, here are some strategies to help you maintain your job.
INFORM YOUR EMPLOYER If you have a condition that could interfere with your performance, tell your boss. People are often afraid of being discriminated against, saidRosalind Joffe, a career coach who counsels people with chronic illnesses. I had one client who didnt disclose his illness to anyone. His odd behavior led his boss to conclude he was a drug abuser.
Be honest. Explain what your condition is and how it might affect your work. Dont be ashamed, Ms. Frechette said.
A supervisor who understands what is wrong is less likely to make false assumptions about what you can and cannot do. Be clear about your value and what you can deliver, Ms. Joffe said. If youre a valued employee, your boss will work with you.
If you feel you are being unfairly treated, speak with your supervisor. If that doesnt work, go to the human resources department.
ASK FOR ADJUSTMENTS If your illness meets the definition of a disability, your employer is required to make reasonable accommodations to your job or work environment, according to the Americans With Disabilities Act.
What is a disability? Its a physical or mental impairment that substantially limits one or more major life activities, said Chris Kuczynski, director of the division that deals with the disability act at the federal Equal Employment Opportunity Commission.
Although your illness may be episodic or controlled by medications, it is still a disability, according to a recent amendment to the law.
Your employer does not have to provide an accommodation if it would impose significant difficulty or expense. Asking for a car and driver to take you to and from work would probably not be reasonable, Mr. Kuczynski said. But taking time off for chemotherapytreatments certainly would.
According to the Society for Human Resource Managers, the top five accommodations for the disability act provided by employers in 2005 (the last year for which data are available) were parking or transportation modifications, making existing facilities accessible, offering new equipment to workers, restructuring jobs and modifying the work environment.
If you are not sure what type of accommodations you are entitled to or how to ask for them, contact the Job Accommodation Network (800-526-7234), a service provided by the federal Department of Labor. In general, the network recommends that you put your request to your employer in writing. If you work in a small, informal setting, that may not be necessary.
KNOW THE TIME-OFF POLICIES You can learn about the on-the-books rules by going to your companys intranet or speaking with its human resources department.
If you need to take a few weeks or months off for an operation, for example, or chemotherapy, research your companys short- and long-term disability plans. Disability policies typically allow you to take a specific time off at reduced pay. According to Mercer, the consulting firm, 78 percent of employers offer short-term plans and 80 percent offer long-term disability plans.
You can also tap into your 12 weeks of family and medical leave at any time. You may take the time intermittently or all at once. You will not be paid, but your job will be secure.
EXPLORE ALTERNATIVES If the hours are too long or the work is too taxing to handle while you are ill, find out whether you could work part time or could even take a different job in your company.
If neither is feasible, explore new career possibilities. One of Ms. Joffes clients was a high-powered lawyer who had a serious heart condition. To reduce stress, he decided to give up litigation and become a teacher.
If you are worried about your finances or health insurance, be sure to check with the advocacy organization focused on your disease. The American Cancer Society, for instance, has a call center (800-227-2345) that helps people who dont have health insurance or are on the verge of losing it.
If your illness finally prohibits you from working altogether, you may apply for Social Security disability insurance. The process is lengthy, and you must be able to prove that you cannot work at any job. The amount you are paid is based on your lifetime earnings you can find the number on the annual statement you receive from the Social Security Administration.
Generally, payments are modest: the average in 2008 was $1,063 a month. But once you have received disability payments for two years, you automatically qualify for Medicarecoverage..
"Remember.Research is the key to your cure!"
Attention: Important Announcement for AIP Study
Friday - August 16, 2013 @ 12:40:08
Alnylam Pharmaceutical will begin research on their new treatmen, ALN-AS1,t for AIP in early 2014. The APF will be working with Alnylam locating patient volunteers etc. ALN-AS1 is a subcutaneous RNAi therapeutic targeting aminolevulinate synthase-1 (ALAS-1) for the treatment of acute intermittent porphyria (AIP), an ultra-rare genetic disease. ALN-AS1 has the potential to be a therapy for the treatment of acute porphyria attacks, as well as a prophylactic approach for the prevention of recurrent attacks. Our first meeting on the subject was very exciting. Plus , the scientists presented a n overrview of the reseach at the International Porphyria Conference I will be meeting again with them in Sept and will tell you all the details. Research volunteers will be needed . If you are interested, contact me as we are beginning a list now please call and contact Desiree Lyons 866-apf-3635. "Remember.Research is the key to your cure!"
Happy & Healthy
Wednesday - August 14, 2013 @ 12:49:21
Have a Happy & Enjoyable weekend to all.
www.porphyriafoundation.com
Be Well, Stay Well
"Remember.Research is the key to your cure!"
Fun Facts: OF PCT SYMPTOMS
Wednesday - August 14, 2013 @ 12:46:32
Did you know: Symptoms of PCT
The most common symptoms of PCT are fragility and blistering of light-exposed areas of the skinespecially the backs of the hands, the lower arms and the face. Patients often report that their skin is unusually fragile, so small bumps or knocks can scrape away the upper layer of the skin or cause a blister. The blisters contain fluid, rupture easily, crust over and then heal slowly. Skin infections, scarring and changes in coloration may result. Small white spots called "milia" are commonly found on the hands and fingers.
Another feature which is often seen is excessive growth of facial hair. The reason for this is not at present understood, but once the disease is under control, the hair can usually be easily and effectively removed by conventional methods. Some patients develop severe scarring and thickening of the skin, which is referred to as "pseudoscleroderma".
PCT is accompanied by some degree of liver damage. This is often mild or moderate. But over time there is a risk of developing cirrhosis and even liver cancer. Liver damage in PCT may be due in part to the excess porphyrins, which accumulate in very large amounts particularly in the liver. But other factors, such as alcohol, Hepatitis C and excess iron, can be important causes of liver damage.
Neurological symptoms, which are common in acute porphyrias, such as pain in the abdomen and extremities, are not features of PCT. "Remember.Research is the key to your cure!"
Please Support the American Porphyria Foundation- We need your help.
Wednesday - August 14, 2013 @ 12:44:08
Support the American Porphyria Foundation
Please support the American Porphyria Foundation today. When you support the APF, you are making a contribution to an organization that provides solid medical information, hope and essential support to those affected by porphyria. You can be proud to be an integral part of the help we provide patients on the road accurate diagnosis, proper care, and hopefully someday a cure.
We welcome donations by phone, mail, fax, or online. Please call us with toll free at 1-866-APF-3635 Monday-Friday from 9:00 a.m. to 4:00 p.m. CST. We accept VISA or Mastercard.
You may choose to honor a friend or loved one with your donation, or to remember someone with a memorial gift.
You can give online with a major credit card via PayPal:
Matching Gifts Many companies offer matching gift programs to encourage their employees to make charitable contributions. Most of these programs match your contribution dollar for dollar, and some will even double or triple the amount of your gift.
To find out if your company will match gifts to the APF, please contact your employer to request their matching gift form and send it to us with your donation.
Financial Information
The American Porphyria Foundation was incorporated in 1983 as a tax-exempt 501(c)(3) organization. All contributions, grants and bequests are tax deductible. Our most recent 990 tax forms are available from the office.
Our work is supported primarily through donor contributions. We do not receive or use government funds.
"Remember.Research is the key to your cure!"
Mobile Web App for Safe/Unsafe Drug List
Wednesday - August 14, 2013 @ 12:43:21
Mobile Web App for Safe/Unsafe Drug List
We sincerely appreciate the hard work of APF member, Mr. Nicholas Frias , who designed a fantastic Mobile Web App for the Safe/Unsafe Drug List for the Acute Porphyrias. He combined the APF list and the European and South African lists to create an easy to search list.
This Mobile Web App is very simple to use. All you need to do is enter porphyriadrugs.com into your mobile device web browser to access it. Follow easy instructions to add the list to your home screen.
The desktop version works well, too. Mr. Frias will be updating the list with the assistance of porphyria expert, Dr. Peter Tishler. There is a comment section to track glitches in the system, so please feel free to add your comments, as Mr. Frias will continue to update the site.
This is a very special gift from Mr. Frias to people who have one of the acute porphyrias. Please join the APF in sending him our sincerest thanks.
"Remember.Research is the key to your cure!"
For Healthcare Professionals
Monday - August 12, 2013 @ 19:15:03
For Healthcare Professionals
This section of the website includes more detailed information about the three most common types of Porphyria: AIP (and the clinically similar HCP, VP & ADP), EPP and PCT. For more general information, please see the About Porphyria section of the site. A more in depth discussion of diagnostic issues in the porphyrias can be found in the Testing and Treatment section of our website.
Clinicians and researchers specializing in Porphyria are available to consult on suspected or confirmed cases of Porphyria, and to discuss the individual course of treatment. Some specialists can assist with diagnostic testing, and some are available for clinical consultation with patients. There is one telemedicine facility for Porphyria consultation in the country, at the University of Texas-Medical branch, in Galveston.
Please call the APF office at 713-266-9617 for information on contacting the specialist who can best answer your concerns.
The APF encourages you to let Porphyria patients know about our organization and our programs. We publish educational brochures, written by Porphyria experts for a lay audience, and a quarterly newsletter in addition to this website. We also offer members a national support network, which for some people provides the first-in-a-lifetime opportunity to speak with someone who shares their diagnosis.
"Remember. Research is the key to your cure!"
APF Newsletter's Past and Present
Friday - August 9, 2013 @ 19:14:21
Please be sure to take so time to read about the American Porphyria Foundation's Newsletters! You can read about Dr. Info expert advice, suggestions, member stories tips on all the types of Porphyria. Click on this link: http://www.porphyriafoundation.com/news/newsletter. If you would love to receive the newsletter in your mailbox please check out how you can become a member today. Contact Yvette @ the American Porphyria Foundation @ 866-APF-3635 or email her today @ Porphyrus@aol.com.
"Remember. Research is the key to your cure!"
Read about our new APF FB Admin Pierre Mouledoux
Wednesday - August 7, 2013 @ 22:55:45
We would love to welcome out new FB Admin to the EPP,CEP group Pierre Mouledoux. I asked Pierre a few questions so that we could all get to know about him & his family. His background is very interesting and also how he has been able to support the
American Porphyria Foundation. Thank you for opening up Pierre and I hope everyone enjoys reading this. Pierre Mouledoux is a licensed real estate agent and the project manager for Sperry Van Ness/Gilmore Auction & Realty Co. in New Orleans. Pierre recently received his Notary commission after successfully passing the Notary examination. He currently serves as State Publicity Chairman for Louisiana Ducks Unlimited State Committee, and is a member of both the Jefferson Parish Ducks Unlimited and New Orleans Ducks Unlimited Committees. Pierre and his darling wife Alyse are expecting their first child due in January 2014. He is also an 2003 Eagle Scout of Troop 230 in Metairie, LA. Having EPP severely limited his passion for the outdoors. Living in south Louisiana and being covered up as the current cure suggests made being outdoors that much more unbearable from the heat, humidity, and obviously the light. After a reaction, a cold dark room with damp towels, ice packs, and hypo-allergenic baby lotion was what was in store for recovery. Pierre was diagnosed with EPP at the age of 7 by an intern at Charity Hospital in New Orleans in 1992 after a long battery of tests in order to determine his light sensitivity. He became active in the EPP community after joining the American Porphyria Foundation and its Facebook groups. He participated in the phase III trials of Clinuvels Scenesse with the real drug and had promising results. The drug allowed him to do the things he loves such as hunting, fishing, and outdoor cooking. He recently attended the FDA meeting in Washington DC to push for the approval of Clinuvels Scenesse and explain the success he had with the drug. Pierre has been made an administrator of the APF Facebook Group EPP/CEP.
"Remember. Research is the key to your cure!"
Please read Urgent 4.5 million grant for Porphyria How you can get involved.
Tuesday - August 6, 2013 @ 11:16:01
The Porphyria Research Consortium has a an excellent chance at winning a $4.5 million research grant but YOU are needed. Unless we can locate enough research patients there can be no research trials. These projects are different than others. All that is required of YOU is to donate some of YOUR blood, swab YOUR cheeks for DNA and answer a questionnaire. There are seven studies in which you can choose to participate. Please contact Hetanshi Naik at hetanshi.caik.mssm.edu or the APF. To be eligible for the Longitudinal Study of the Porphyrias: Must have a confirmed diagnosis of one of the porphyrias It is preferable if patients are able to come to a participating center to be clinically evaluated (through insurance if possible) If patients cannot come to a center they can be seen by a local physician and have their records sent to a participating center along with the necessary samples (DNA, porphyria labs, etc) To participate in the following studies the patient MUST already be in the Longitudinal Study: Erythropoietic Protoporphyrias: Studies of the Natural History, Genotype-Phenotype Correlations, and Psychosocial Impact Mitoferrin-1 Expression in Patients with Erythropoietic Protoporphyria Quantification of the Effects of Isoniazid Treatment in Erythrocyte and Plasma Protoporphyrin IX Concentration and Plasma Aminolevulinic Acid in Patients with Erythropoietic Protoporphyria To participate in Clinical Diagnosis of Acute Porphyrias, there are two parts: Part 1 is looking for 1st degree relatives of patients with confirmed DNA diagnoses of the acute porphyrias (the patients who are subsequently diagnosed with an acute porphyria through this study are then eligible to participate in the Longitudinal Study)- We are only recruiting for this part right now Part 2 is looking for patients with mild elevations in urine porphyrins and symptoms consistent with acute porphyria but who do not have a confirmed diagnosis yet (again, patients who are subsequently diagnosed with an acute porphyria through this study are then eligible to participate in the Longitudinal Study) For this study patients do not need to visit a participating center but it is preferred that they do To participate in Hydroxychloroquine vs. phlebotomy for porphyria cutanea tarda : Patients must have a biochemically confirmed diagnosis of PCT, these patients are also eligible to be in the Longitudinal Study however it is not required that they be in the Longitudinal Study to be in this study They must also be over 18 years of age and willing to take precautions to prevent pregnancy For this study the patients need to visit a participating center CALL THE APF IF YOU WOULD LIKE FURTHER INFO AND ASK FOR DESIREE OR EMAIL HETANSHI NIAK AT THE Mount Sinai Medical School in NYC @ hetanshi.naik@mssm.edu "Remember. Research is the key to your cure!"
International Porphyria Patient Day Read all about it!
Video and Audio of the International Porphyria Conference are available by joining RareConnect.org.
On the video, representatives from patient groups introduce themselves; tell about the organizations in their respective countries and share patient testimonials.
Porphyria Argentina - Estela Y. Ferrari de Frassia
Enter as a Guest with your Name, no password required. Connect your headset.
Mission:"People living with EPP and their families come together to share their stories, realize their similarities, share their strategies, and have a virtual meeting. There will be plenty of time for discussion."
"Remember. Research is the key to your cure!"
Here is an experience with Children with EPP! This has been brought to you by Rare Connect.
Monday - July 29, 2013 @ 16:19:22
Bringing up 2 Children with EPP
Listed below is the brief story of our journey with EPP.
We have 3 teenage children. the two eldest have EPP and the youngest carries the gene. We first noticed problems with our two eldest on holidays to Spain when even when not in the sun and covered with factor 50, they complained of burning hands. Both my daughter and son suffered scarring and skin flaking away from their hands and feet and in one very alarming incident my daughters face blew up like a balloon and the skin across it split.
We naturally started to consult medical professionals very quickly, but it took about 3 years for the full diagnosis to come through. Once we had the diagnosis of EPP the children attended Hope Hospital in Manchester where their care has been excellent.
It has meant us making some changes to the way we live our lives to ensure that they are both protected from the sun, but over time they have learnt to manage their condition within reason. They keep well covered, in the shade and when we holiday they swim in early evening or we choose hotels with indoor pools. Though I must admit looking back at pictures of them sitting in the sun in their early years makes me shudder now that I know what it must have been doing to them, even with hats and sun cream on.
We are still looking to erradicate EPP from their lives and potentially from the lives of their children when the time comes. Seeing them struggle with burnt and cracked hands and faces has been horrible and not something I want to see again.
The conference in Luzern was a huge step forward in our understanding of Porpyhria, its short term and long term impacts and also potential treatments and it was well worth the trip and all the effort put in by everyone to organise it. So many thanks to Rocco and Jasmine.
"Remember.Research is the key to your cure!"
How Does a Heat Wave Affect the Human Body?
Sunday - July 28, 2013 @ 19:37:05
Excellent and informative article I had to share.
How Does a Heat Wave Affect the Human Body?
Some might like it hot, but extreme heat can overpower the human body. An expert from the CDC explains how heat kills and why fans are worthless in the face of truly high temperatures
CAN WE REALLY BEAT THE HEAT?: The human body can face a meltdown if exposed to a prolonged heat wave. Heat exhaustion and heat stroke are just some of the effects of hot weather on the body.Image:
Climate change promises to bring with it longer, hotter summers to many places on the planet. This June turned out to be the fourth-hottest month ever recordedgloballyscientists are reporting. With more heat waves on the horizon, and a big one currently sweeping much of the U.S., the risk of heat-related health problems has also been on the rise.
Heat exhaustion is a relatively common reaction to severe heat and can include symptoms such as dizziness, headache and fainting. It can usually be treated with rest, a cool environment and hydration (including refueling of electrolytes, which are necessary for muscle and other body functions). Heat stroke is more severe and requires medical attentionit is often accompanied by dry skin, a body temperature above 103 degrees Fahrenheit, confusion and sometimes unconsciousness.
Extreme heat is only blamed for an average of 688 deaths each year in the U.S.,according to the Centers for Disease Control and Prevention (CDC). But when sustained heat waves hit a region, the other health ramifications can be serious, including sunstroke and even major organ damage due to heat.
The Chicago heat wave in the summer of 1995 killed an estimated 692 people and sent at least 3,300 people to the emergency room. An observational study of some of those patients revealed that 28 percent who were diagnosed at the time with severe heat stroke had died within a year of being admitted to the hospital, and most who initially survived the high temperatures had "permanent loss of independent function," according to a 1998 study of the heat wave, published in Archives of Internal Medicine.
As temperatures linger above our bodies' own healthy internal temperature for longer periods of time, will we humans be able to take the heat? We spoke with Mike McGeehin, director of the CDC's Environmental Hazards and Health Effects Program, to find out just whyand howa warm, sunny summer day can do us in.
How do humans cope with hot, hot weather? The two ways we cope with heat are by perspiring and breathing.
So is it the heat or humidity that is the real killer? The humidity is a huge factor. If you have tremendously high temperatures and high humidity, a person will be sweating but the sweat won't be drying on the skin. Thats why it's not just heat but the combination of heat and humidity that matters. That combination results in a number called the apparent temperature or "how it feels".
Obviously there are thresholds for both temperature and humidity above which we see an increase in death, and it's going to be a different temperature in Phoenix than it's going to be in Chicago.
The other major factor in terms of temperature that causes both mortality and morbidity is the temperature that it falls to in the evening. If the temperature remains elevated overnight, that's when we see the increase in deaths. The body becomes overwhelmed because it doesn't get the respite that it needs. What kind of impact does extreme, sustained heat have on the human body? The systems in the human body that enable it to adapt to heat become overwhelmed. When a person is exposed to heat for a very long time, the first thing that shuts down is the ability to sweat. We know that when perspiration is dried by the air there is a cooling effect on the body. Once a person stops perspiring, in very short order a person can move from heat exhaustion to heat stroke. What happens in the transition from heat exhaustion to heat stroke? It begins with perspiring profusely, and when that shuts down, the body becomes very hot. Eventually that begins to affect the brain, and that's when people begin to get confused and can lose consciousness.
The analogy we use is if you're driving a car and you notice that the temperature light comes on, what's happening is the cooling system of the car is becoming overwhelmed. If you turn off the car and let it cool eventually you can start driving again. But if you continue to drive the car, the problem goes beyond the cooling system to affect the engine, and eventually the car will stop.
What other areas of the body does this extreme overheating affect? As the body temperature increases very rapidly, the central nervous system and circulatory system are impacted.
In places where there have been prolonged heat exposures, there is probably a broad impact on many organ systems. From heat waves that have been studied, like in Chicago, there are increases in emergency department visits and hospital stays for medical crises that are not normally associated with heat, such as kidney problems.
But it really hasn't been studied very much. One of the reasons for that is the main focus of the studies has been on mortality from heat waves, and there hasn't been that much focus on morbidity. That would take looking at people who are hospitalized from heat exhaustion or heat stroke and following them into the future.
Before someone gets full-blow heat stroke, what are the body's early reactions to excessive heat? Heat rash andmuscle crampsare early signs of people being overwhelmed by heat. If those aren't dealt with, it can lead to more severe symptoms.
Cramping of muscles can be for a number of different issues, including electrolytes not getting to the muscles.
People should be aware that their skin turning red and dry are indicators that heat is impacting them.
Who is the most vulnerable to extended high temperatures? We know the risk factors for dying from heat are urban dwellers who are elderly, isolated and don't have access to air conditioning. Obese people are at increased risk as are people on certain medications. And people who are exercising or working in the heat, who don't meet those criteria, can be at risk. What medications can make the body more susceptible to extreme heat? In the study from the 1995 Chicago heat wave, we found that diuretics for high blood pressure were some that did, and beta blockersa number of studies showed that people taking them could be at increased risk.
There are some studies that have shown that certainmental healthmedications may impact a person's ability to deal with the heat. But that's a difficult one to get at. When you look at the number of people who die in a heat wave and the number of people who are taking those medications, the numbers can get pretty small pretty quickly. What's the hottest temperature a healthy human can tolerate? We don't know thatno one knows that. There are different humans, different humidities, different types of temperature. Have we not evolved to cope with super hotweather? Certainly society has evolved in dealing with the heatand that has been in the development of air conditioners. The number-one factor that ameliorates death from heat is access to air conditioning.
And I've read that fans don't work to prevent overheating in really hot temperaturesâ?¦ Not only does it not work, it actually makes it worse. We compare it to a convection oven. By blowing hot air on a person, it heats them up rather than cools them down.
Are modern humans neglecting to do something our ancestors did to survive the heat? I think it's always been a problem. There's history over hundreds of years of people dying of heat. Philadelphia in 1776 had a major heat wave that caused deaths.
We're also living to older ages, and we're more urban now than we have been in the history of the human species. That intense crowding can combine with the heat island effect in big cities. Our elderly people are also more isolated than they have been in the past, so those factors can play a part, too.
The IPCC, the Intergovernmental Panel on Climate Change, the thing that they are most comfortable in predicting, that the science is most solid for, isthe increasein many parts of the world in the duration and intensity of heat waves.
Everyone!!!! **** The T-shirts are almost all gone here is what I have left in sizes: XL-1XL= 12, L-1, M-12, S-7, so if you would like to place an order leave your order @ porphyriaorders@gmail.com along with method of payment and full mailing address. We accept Visa, MC, Money order and personal check. http://www.porphyriafoundation.com/news/APF-T-Shirts
"Remember.Research is the key to your cure!"
Fruits & Veggies Then & Now
Wednesday - July 24, 2013 @ 11:24:56
I found this really interesting. I am a big fan of fruits and veggies. I encourage you to read this over.
Are Fruits and Vegetables Less Nutritious Today?
Studies suggest that today's fruits and vegetables might be missing some key nutrients. Find out why, and discover shopping and cooking techniques that preserve nutritional value.
A number of studies have explored the phenomenon of declining nutrients in fruits and vegetables, but the one that garnered the most media attention was led by Donald R. Davis, PhD, at theUniversity of Texas in Austin, and was published in HortScience. Among Daviss findings, one of the most consistent was that a higher yield of crops in other words, more crops grown in a given space almost always resulted in lower nutrient levels in the fruits and vegetables. Whats more, the median mineral declines among a variety of fruits and vegetables could be fairly significant, ranging from 5 to 40 percent, with similar declines in vitamins and protein levels.
Higher yield is one reason behind the decline, but severalnutrition experts say it's not the only one. The soil itself has been over-harvested, meaning that over years of use and turnover of soil, it becomes depleted in nutrition, says Michael Wald, MD, an integrated medicine specialist in Mount Kisco, N.Y. All crops growing upon depleted soil must therefore be depleted in nutritional content.
Cherie Calbom, MS, a clinical nutritionist and author of The Juice Lady's Living Foods Revolution, sees it as a bigger problem that extends to many aspects of modern farming. Our poor farming practices are leading to sick plants, depleted soil, and a need to use higher and higher doses of pesticides and herbicides to ward off what healthy plants would naturally ward off, she says. We are heading toward a dust bowl in many parts of the country if nothing changes.
Despite these concerns, Janet Brill, PhD, RD, a nutritionist and author of Cholesterol Down, its still critically important to eat lots and lots of fruits and vegetables, and these developments shouldnt discourage you from doing just that. People should be concerned about one area of fruits and vegetables and one area only: to eat lots more of them each day, cooked and raw, she says. After we have solved that problem [of consumption], then we can move on to any nutrition concerns about growing them.
5 Ways to Get the Most Out of Your Fruits and Veggies
There are still many steps you can take to ensure a healthy nutrient punch every time you include fruits and vegetables in your diet.
Go with locally grown. The key to getting more nutrients is eating food that spends less time traveling from the field to your table. The way to accomplish that goal is with locally grown produce, either from your own garden or from a local farmers market. Buy fresh, whole, and locally grown seasonal produce, Brill suggests. Try to purchase produce with the least amount of time from farm to table, as vitamins and minerals are lost over time as well as with cooking and handling.
Choose frozen. Your natural instinct when eating produce is to think that fresh is always better than frozen. But Brill says that this isnt necessarily the case. Sometimes the veggies frozen right after harvest have retained more nutrients than those fresh veggies that have taken forever to get to your plate, she explains.
Dont judge a book by its cover. Big, shiny fruits and vegetables sure look good and grab your attention in the supermarket, but just because theyre beautiful doesnt mean theyre better for you. For example, organic apples may be smaller and not quite as pretty, but their pesticide levels are likely to be lower.
Keep them rough. When it comes time to prepare those fruits and vegetables for eating, bigger, rougher pieces of produce may have the nutritional edge over finely chopped and sliced options. Keep chopping to a minimum, Brill advises. The greater the exposure of the fruit or vegetable to air, the greater the loss of nutrients.
Minimize cooking time. Though there are some exceptions (the lycopene in tomatoes, for example), the less most fruits and vegetables are cooked, the more nutrients they retain. So eat your fruits and vegetables raw whenever possible. When you do cook them, keep the cooking time to a minimum and avoid too much contact with water. Cooking methods that are quick, with a minimum amount of liquid, will help to preserve nutrients, Brill says. Steaming, blanching, and stir-frying are all great ways to cook vegetables quickly and retain valuable nutrients. Keep veggies crisp never overcook or boil in water until soggy.
It may take a bit more effort to find fruits and vegetables as nutrient-rich as they were 50 years ago, but with more local farm stands cropping up, seasonal choices are getting easier to find and are certainly more delicious.
"Remember.Research is the key to your cure!"
Big News Reports from the American Porphyria Foundation
Tuesday - July 23, 2013 @ 21:17:38
The APF Website has Received a Makeover.
We are pleased to announce the release of the Updated APF website.
Some of the new sections Include:
New Rotating Members Photo's and Quotes Gallery on the Home Page.
New "Porphyria Awareness and Fundraising Events" section with both Past and Present Events.
New informative Videos on the Home Page and You Tube videos on a variety of subjects.
New links to special educational sections
And a host of other informative resources
An enhanced Image Gallery.
Additional Member and Panhematin stories.
Previews of the video, Porphyria Live and much more
Take a look and we hope you all benefit from the vast resource of Information. Note the medical information on the APF website was written by Porphyria Experts: http://porphyriafoundation.com. .
Watch the website for more exciting new features which will be added over the next month, including easy access to Desiree's book, Porphyria , A Lyon's Share of Trouble and an Art Gallery of our members talent.
Please submit your own stories, paintings, poetry, and videos or You Tube videos. The APF is your foundation. We want to add more about you. Contact Yvette at the APF at porphyrus@aol.com or call 866.apf.3635.
NEW Caretaker Support Forum.
Warren Hudson, who serves on the APF Board of Directors, has agreed to head our Caretaker Support Forum for spouses or partners who help their loved one cope with porphyria. To read more about Warrens story as a caretaker for a loved one with AIP view here.
The Caregiver Support Group strives to provide a forum to ask questions, share advice, experiences and provide a sounding board for those going through similar circumstances.
Our goal is to eventually provide multiple resources to assist caregivers in their day-to-day lives. This is your community and your input will help shape this service. Whether you are a spouse, partner, relative or friend of a porphyria patient, we want to hear from you. Contact the American Porphyria Foundation or email us at apfcaregiver@aol.com for more information.
We respectfully request that only caregivers of patients in the active process of diagnosis or with a diagnosis of a porphyria participate in this group.
Official APF T-Shirts are Still Available.
Thank you to all of you who have already purchased their APF T-Shirts and Porphyria Live DVD's. The interest you all have shown is very exciting for us.They are going fast. Order yours today! For instructions on how to order yours view here.
New Safe/Unsafe Drug List Mobile Web App.
We sincerely appreciate the hard work of APF member, Mr. Nicholas Frias , who designed a fantastic Mobile Web App for the Safe/Unsafe Drug List for the Acute Porphyrias. He combined the APF list and the European and South African lists to create an easy to search list. Read more
"Remember.Research is the key to your cure!"
Summer vacation a personal experience from Natalia Nikova
Tuesday - July 23, 2013 @ 21:06:15
It's summer time have you taken a vacation yet? Please read the reminders off a new personal experience from Natalia Nikova
Type of Porphyria:
Acute Intermittent Porphyria (AIP)
Beware of Mountains
My name is Natalia Nikova. I was born in Russia in St. Petersburg. I have AIP.
I went through horrible surgeries and sufferings in Russia before I was properly diagnosed. That happened when I was between 25 and 30 years old.
After that I was receiving capsules of Adenil through the Red Cross for about four years and injecting myself two times a day. My recovery was very slow but at the age of 39 I started to feel better and I was able to immigrate to the USA with my daughter and my mother.
I managed to change my profession from Choral conductor to a computer programmer to support my family and my porphyria's symptoms almost disappeared. Now I am 63 years old and in August 2004 all of a sudden I had a reminder. I and my husband went to Peru. I got immediately sick in Cusco from the high altitude but the altitude sickness was greatly aggravated by porphyria. In addition to a headache and shortness of breath I had nausea, high fever, high blood pressure and grazing pain in my stomach. In fact I became so sick that we had to change our entire itinerary and move to lower regions in Peru. That was not too much fun because I am a bird watcher I was looking forward to go to Colca Canyon to see Andean Condor. Even after we returned from Peru I was sick for two weeks with general weakness.
I hope that sharing this story will help some people in planning their vacation.
"Remember.Research is the key to your cure!"
FDA Warns of Sunscreen Spray's Flammability Risk
Friday - August 23, 2013 @ 18:24:42
FDA Warns of Sunscreen Spray's Flammability Risk
SUNDAY, July 21 (HealthDay News) -- Certain sunscreen sprays worn close to an open flame may pose a risk of catching fire, the U.S. Food and Drug Administration warns.
The agency said it knows of five incidents in which people wearing sunscreen spray near sources of flame suffered significant burns that required medical treatment. The products involved in these incidents were recalled and should no longer be on store shelves.
However, many other sunscreen spray products contain flammable ingredients, commonly alcohol. The same is true for some other spray products -- including insect repellants and hairsprays -- and even some non-spray sunscreens, the FDA said.
"Based on this information, we recommend that after you have applied a sunscreen spray labeled as flammable, you consider avoiding being near an open flame, sparks or an ignition source," Dr. Narayan Nair, a lead medical officer at the FDA, said in an agency news release.
Many flammable products have a label warning against their use near an open flame. Never apply a product labeled as flammable when you are near a source of flame.
However, the five incidents reported to the FDA occurred after the sunscreen spray had been applied. The sources of flame included lighting a cigarette, standing too close to a lit citronella candle, approaching a barbecue grill and doing welding.
These incidents indicate that catching fire is possible even if you believe you have waited long enough for the sunscreen to dry and your skin feels dry, the FDA said.
"Remember.Research is the key to your cure!"
New shipment arrived today! APF-T-shirts & APF videos selling out get yours today.
Thursday - July 18, 2013 @ 13:09:47
Back by popular demand! New shipment in. These will not last long. They are going quick. Did you get your video & T-shirts yet? Support the APF by making your purchase today!
We are pleased to announce that the official APF T-Shirts have arrived!
Our hope for the T-shirts is that you all will buy and wear them to help promote and raise questions about Porphyria and to raise funds for the Dr. Packets, pain Management docs, among many other publications we make available at no cost.
Amy Chapman is heading up the T-shirt project. There are also some copies of Porphyria Live for sale. For information on how to order the T-Shirts and/or the Porphyria Live Video see below.
Porphyria Live DVD Introduction
You can order a T-shirt and/or Porphyria Live DVD by sending an email order toporphyriaorders@gmail.com
I must have name, complete address, and phone number. Also include the Quantity of T-shirts and the size for each one. And include the quanity of the Porphyria Live Video.
To accept payment: One of two options I can accept Paypal VISA/MC only I must have full name on the card, account#, exp. date, 3 digit code on back of card CVV-
I will accept money orders and personal checks. You must have name/address/phone # on them.
They can be mailed to me:
Amy Chapman
10475 Gandy BLVD N. Unit 3417
St. Petersburg FL 33702.
*The APF will not take orders or calls about T-shirts*
Once I receive the order I will ship out your product.
All products will be shipped out Priority mail with tracking. Each person also will receive a receipt with T-shirts.
T-shirts come in the following sizes S, M, L XL, 2xl, 3xl they are 100% cotton, heavy not thin, and very durable. No other sizes.
The price per T-shirts is $19.00/shirt. This covers the shirt, shipping and tracking, and priority mail. International orders: I will have to consult first with the post office for shipping rates.
The price of the Porphyria Live DVD is $10.00 each. Shipping is included in the price.
100% of all funds received will go back to the APF
"Remember.Research is the key to your cure!"
APF Website received a makeover! Check it out.
Wednesday - July 17, 2013 @ 11:29:00
The APF Website has received a makeover! Take a look at some of our new features like the New Rotating Members Photo's and Quotes Gallery on the Home Page.
There is a new section "Porphyria Awareness and Fundraising Events" A list of Past and Present Events.
Among many other things. Take a look and we hope you all benefit from the vast resource of Information provided and screened by Porphyria Experts.
The APF Website has received a makeover! Take a look at some of our new features like the New Rotating Members Photo's and Quotes Gallery on the Home Page.
There is a new section "Porphyria Awareness and Fundraising Events" A list of Past and Present Events.
Videos on the Home Page, Among many other things.
Take a look and we hope you all benefit from the vast resource of Information provided and screened by Porphyria Experts.
Enter as a Guest with your Name, no password required. Connect your headset
Mission: People living with EPP and their families come together to share their stories, realize their similarities, share their strategies, and have a virtual meeting. There will be plenty of time for discussion.
We hope you can join us on August 11! If you're on holidays, don't worry, we'll record it and post the video here afterward.
"Remember.Research is the key to your cure!"
Offical APF T-Sirts Ordering Information below. Order your TODAY.
Tuesday - July 16, 2013 @ 20:59:49
We are pleased to announce that the official APF T-Shirts have arrived!
Our hope for the T-shirts is that you all will buy and wear them to help promote and raise questions about Porphyria and to raise funds for the Dr. Packets, pain Management docs, among many other publications we make available at no cost.
Amy Chapman is heading up the T-shirt project. There are also some copies of Porphyria Live for sale. For information on how to order the T-Shirts and/or the Porphyria Live Video see below.
Porphyria Live DVD Introduction
You can order a T-shirt and/or Porphyria Live DVD by sending an email order toporphyriaorders@gmail.com
I must have name, complete address, and phone number. Also include the Quantity of T-shirts and the size for each one. And include the quanity of the Porphyria Live Video.
To accept payment: One of two options I can accept Paypal VISA/MC only I must have full name on the card, account#, exp. date, 3 digit code on back of card CVV-
I will accept money orders and personal checks. You must have name/address/phone # on them.
They can be mailed to me:
Amy Chapman
10475 Gandy BLVD N. Unit 3417
St. Petersburg FL 33702.
*The APF will not take orders or calls about T-shirts*
Once I receive the order I will ship out your product.
All products will be shipped out Priority mail with tracking. Each person also will receive a receipt with T-shirts.
T-shirts come in the following sizes S, M, L XL, 2xl, 3xl they are 100% cotton, heavy not thin, and very durable. No other sizes.
The price per T-shirts is $19.00/shirt. This covers the shirt, shipping and tracking, and priority mail. International orders: I will have to consult first with the post office for shipping rates.
The price of the Porphyria Live DVD is $10.00 each. Shipping is included in the price.
100% of all funds received will go back to the APF
"Remember.Research is the key to your cure!"
Feelings~ This is how I feel sometimes
Monday - July 15, 2013 @ 23:31:36
"Remember.Research is the key to your cure!"
Warren Hudson ~ Caretaker
Tuesday - July 23, 2013 @ 10:28:39
Warren Hudson ~ Caretaker
Type of Porphyria:
Acute Intermittent Porphyria (AIP)
Warren Hudson, who serves on the APF Board of Directors, has agreed to head our Caretaker Support Forumfor spouses or partners who help their loved one cope with porphyria. If you would like to participate in the Caretaker group, please contact the APF for Warren's contact information. Below is Warrens story.
"Porphyria is a large part of my life effecting relationships and day-to-day activities. It controls my ability to work, what kind of jobs I can take, and how I care of my family. Porphyria cost me friendships and takes a great mental and physical toll. I am extremely afraid of the simple act of visiting new doctors. I go prepared with questions and the expectation of disappointment or rejection. The horror related to a hospitalization is something I am unable to put into words. I know my story is common for those suffering with one of the Acute Porphyrias. However, I do not have Porphyria. I am the husband and caregiver of someone with Acute Intermittent Porphyria (AIP). My experience lacks the physical pain but gives me a front row seat to hers and confronts me with an overall feeling of helplessness.
The role of caregiver for a Porphyria patient has been largely unexplored. Obviously, the patient is everyones primary concernas they should be our focus. However, a strong healthy caregiver provides better long-term support. It is all too easy for both caregiver and patient to focus on the patient. In my case, this comes with consequences. At first, both my wife and I treated AIP as something separate from our relationship and our lives. This was unrealistic and fed many disappointments for both of us when we realized the disorder could not be ignored. We strive to understand how it is part of our lives and work together to limits its effect. I wanted to share some experiences, provide insight and hopefully help others in my position.
My wife and I were friends since the age of fourteen, and AIP was never a topic of conversation. I vaguely remember her talking about a hospitalized cousin with extreme pain, paralysis and an undiagnosed illness. However, this was a passing conversation in our mid-teens. Fifteen years after we initially met, her AIP symptoms started. I saw my future wife get increasingly depressed and her frustration build. Often, I was the closest person around taking the brunt of her anger and frustration. In these instances the caregivers role can be very lonely.
In 2003 my wife had an extremely bad attack. I ended up taking off of work for a month, sleeping on the floor next to her in the hospital and being my wifes advocate with nurses and doctors when she was unable to speak for herself. Over the years, this scene has replayed numerous times. I had hospital doctors tell me my wife was faking her symptoms or the pain she described was not possible. I have been called an enabler and accomplice. Despite this, I attempt to continue to advocate for my wifes care and ensure medications are appropriate and her needs met. In extreme cases, I document everything from the time a nurse walks in the room, take pictures of allergic reactions, list medications given and what was said by whom. Every time I go through this process it causes me profound sadness. It seems like an injustice that anyone should have to jump through these hoops to ensure medical care is adequate. I end up feeling like an administrator rather than a husband, but I have caught too many mistakes to stop.
A few months ago I had the opportunity to have breakfast with another husband of an AIP patient. In a year I speak with doctors, healthcare providers, insurance personnel and other Porphyria patients, but rarely do I get to speak to a fellow caregiver. We shared our experiences, fears, and frustrations. The ability to just talk and listen without judgment was cathartic. In these moments, I am reminded my wife and I are not the only people dealing with these issues. No matter how bad it seems, there is someone else who has gone through something similar. Several years ago I was part of a group of patients and spouses sharing our experiences with the makers of Panhematin. I was struck with how familiar each patients story sounded. Away from the group, a few spouses and I shared some of the burdens AIP placed on each of our relationships. These too sounded very familiar.
Every relationship has stresses, but AIP presents some that are new and amplifies others. One of my biggest problems has been its effect on my career. I was offered a position with a company in the United Arab Emirates, and had to turn it down because their Ministry of Health would not allow my wife into the country due to medications she might require. AIP affected our ability to travel to visit friends or take vacations. The risk my wife would become ill and need treatment while on the road is ever-present. We lost friends who felt they were blown off because we did not travel to see them. Some of our friends did not understand why, during periods when my wife was extremely ill, we failed to call or write. Even some family withdrew because they simply did not understand our limitations.
I think one my biggest problems, and generally Porphyria caregivers, is that we do not talk enough to others in a similar position. We tend to hold back, bottle up our emotions, focus on our loved ones and in my case, internalize my frustrations and fears. This can be isolating and unhealthy. I took my personal concerns, pains or illnesses and measured them up against what my wife experienced. In comparison, my problems seemed petty. If I got sick, I treated my illness like something I should push through or shrug off. If I physically could not go to work or do something for my wife I felt guilty because I knew she got out and did things when a day before she was unable to walk. My focus on caring for my wife and not caring for myself affected my health. I gained a large amount of weight and became increasingly depressed.
Even when those closest to me were concerned and wanted to talk, I held back details because it felt like I was betraying my wife by discussing her AIP and how it affected me. I am not suggesting these are common experiences of all caregivers, but as a patient, realize these people by your sides are not passive observers but right there in the trenches with you. It is very easy for those of us in the caregivers role to become immersed in the problems of our loved one and neglect ourselves.
The irony of putting someone elses needs ahead of your own is that both people suffer. It is critical that those of us in the caregiver role take the time to ensure our own needs are being met and that we do not neglect the most important person, ourselves. In order for our spouses, family, friends or loved ones to get the care they need it is imperative that we take care of ourselves both mentally and physically. Reach out to other caregivers if you need advice or a sympathetic ear. Get involved in things that bring you joy. These have been hard lessons for me to learn, and something I struggle with on a daily basis. If you remember anything else, please know neither the patient nor the caregiver is alone in this journey."
"Remember.Research is the key to your cure!"
How to Become a Very Healthy Person-Total Body, Mind, Makeover You deserve it!
Wednesday - July 10, 2013 @ 17:10:30
What great suggestions! Total Body, Mind, Makeover You deserve it! Feel Well Everyone
Want to become a healthier person? It's all about making gradual changes. Following the tips in this article offer several benefits for you: lower risk of several cancers and diseases, a possibly leaner frame, and the chance to live a long and happy life.
1
Get lots of sleep. In order to maintain a healthy body, you'll need 8-10 hours of sleep every day. This keeps you awake and alert, so you don't have to drink caffeine and sugar-loaded energy drinks. If you are a kid and have early school times, go to sleep earlier on school nights.
2
Laugh and smile! Smiling a lot makes your face look younger and it feels great. If you laugh a lot, it has been scientifically proven to keep you healthier.
3
Do nothing. Staying in a dark, quiet place without having any stressful thoughts for about ten minutes will leave you feeling refreshed. If you just relax, you will feel better and probably keep feeling good through the day. Just do this a couple of times a day.
4
Eat more fruits and vegetables. Fruits and vegetables are an essential part of a healthy diet. Try to get at least 5-9 servings a day.
5
Drink water! Good old H2O is key in making you run throughout the day. Try drinking 8 eight-ounce glasses of water each day. It helps you re-energize and keep going. Not drinking enough fresh water leads to acne, headaches, and even dehydration. Do this, and you'll stay in good condition.
6
Stretch! It feels great! From when you wake up in the morning, to your gym class, this easy form of muscle exercise warms you up and makes you more flexible. If you continuously stretch each day, you will end up being really flexible and nimble. It keeps you running longer and gives you strength.
7
Run and jog! This doesn't necessarily mean run five miles every morning, but jogging or running for about 10 minutes at an easy pace definitely will keep you in shape. Try jogging for about 10 minutes 2 times a week. It will keep your muscles strong and fit every day. Don't ever run for an hour and then suddenly stop and sit on the couch for another hour. This will give you terrible cramps and will make it so it hurts to walk the next day. Slowly kick down the pace to a walk, and take deep breaths. Running will get you that A in gym class, trust me!
8
Challenge yourself. If you got 10 push-ups as your maximum, try going for 12! Little challenges like this keep your body nice and fit.
9
Do something you love. Play with a pet, go swimming, or jump on a trampoline! Doing things you love to do keep you in a good mood, and make you happier. If you had a bad day at school, ride a bike and take out your anger. Not only is this fun, but it lets you be yourself for awhile. Try it!
10
Feel good about yourself! There is always going to be someone in the room who does at least one thing better than you, so don't compare yourself to other people! Find things you are good at, and use your talents!
11
Accomplish something. This will make you feel victorious! Performing a song or using your talents to amaze someone else makes you feel great!
12
Get a little exercise everyday. This will not only make you feel better, and make you look better, but help you to get through the day.
13
Be cool - Don't take things too seriously! Be laid-back and open minded, explore new things, e.g. new cultures.
"Remember.Research is the key to your cure!"
Do you have a Service Dog, Companion Dog or a Pet?
Monday - July 8, 2013 @ 10:35:00
Do you have a Service Dog, Companion Dog or a Pet?
Since I have Acute Intermittent Porphyria and have two loving & loyal Service Dogs they are so very important to me, they keep me protected, they can sense danger or harm sometimes before I can even tell if something is going to happen and sometimes we just play and hang out. A few years ago we decided to have pets in our home, my husband never had pets when he was growing up but I grew up with Dogs & Cats. So we decided to adopt from our local shelter. I'm sure some of you can imagine how appreciative and loyal they are. At the time of adoption though it was tough from training, discipline, keeping them clean and so much more. It took so much time and effort sometimes I wondered "Is it really worth it" after all Dogs just wanna have fun! Mixed in with a rare and painful disease I was not always up and ready to go like them. My husband helped out so much to but I was worried. My dogs in the end, from puppies to adult and senior I can say they have helped us through the difficult times. From keeping an eye on me, alerting my husband if something is wrong, opening doors, laying with me when I just want to give up at times, a loyal look, a wagging tail and so much love just as they like to receive love and affection they love to give it. They will be with you in your heart always. So if you need a fellow mate who can help you, think about your circumstances. See who you can share your love with and how your will have a forever "doggie mate".
Service/Assistance Animals
What is a Service Animal?Service animal means any dog that is individually trained to do work or perform tasks for the benefit of an individual with a disability, including a physical, sensory, psychiatric, intellectual, or other mental disability. Other species of animals, whether wild or domestic, trained or untrained, are not service animals for the purpose of this definition. The work or tasks performed by a service animal must be directly related to the handlers disability. Examples of work or tasks performed include, but are not limited to, assisting individuals who are blind or have low vision with navigation and other tasks, alerting individuals who are deaf or hard of hearing to the presence of people or sounds, providing non-violent protection or rescue work, pulling a wheelchair, assisting an individual during a seizure, alerting an individual to the presence of allergens, retrieving items such as medicine or the telephone, providing physical support and assistance with balance and stability to individuals with mobility disabilities, and helping persons with psychiatric and neurological disabilities by preventing or interrupting impulsive or destructive behaviors. The crime deterrent effects of an animals presence and the provision of emotional support, well-being, comfort, or companionship do not constitute work or tasks for the purpose of this definition. (Service animal as defined by the ADA, Title III, subpart A 36.104 definitions, July 2010) All service dogs are granted access by Federal and state laws.
Service Dog Categories
Service dog which assists an individual who has a mobility impairment with tasks including, but not limited to, providing balance and stability, retrieving items and pulling wheelchairs. Dog Guide which assists an individual who is blind or visually impaired with tasks such as, but not limited to, aiding in navigation and alerting the individual to dangers such as moving cars. Hearing Dog which assists an individual who is deaf or hearing impaired by alerting the individual to the presence of sounds or people. Alert/Response Dog which alerts an individual to a seizure or other medical condition. Psychiatric Service Dog which aids an individual with a cognitive, psychiatric or neurological disability.
Therapy dogs, emotional support dogs and companion dogs are NOT service dogs under the ADA.
What Is the Difference Between a Service Dog and Therapy, Emotional Support or Companion Dog?
A service dog must be individually trained to perform work or tasks directly related to the handlers disability. A therapy and emotional support dog merely provides comfort to an individual in some fashion. Therapy dogs are often the pets of the therapist or psychiatric personnel of the particular institution or hospital where they bring comfort. Therapy and emotional support dogs are allowed in housing under the Fair Housing Act (FHA), but are not permitted in public places as are service dogs.
Companion dog is just another name for a pet dog.
Is It a Service Animal? or What questions can be asked?
A service dog is not required to wear something identifying it as such. However, most service dogs wear a vest/cape or harness identifying it as a service dog or dog guide. Service dogs may be of any size. Certification cards are not required. Avest or other identifying clothing is not required. Under the ADA, one may ask if the dog is a service dog and may ask what tasks the dog performs for the handler. One may ask if the handler has a disability, but may NOT ask what that disability is.
Service Animal Behavior (standards as set forth by ADI)
Under the ADA, a service dog may be removed from a public place for disruptive behavior. A service dog must be under the control of the handler at all times. A service dog must be on a leash at all times (some allowances are made under certain circumstances). A service dog must not show aggression towards people or other animals. A service dog does not bark, growl or whine. (However, a service dog may be trained to bark in the case of an emergency effecting the handler) A service dog does not solicit attention, food or other items from the general public, nor annoy any member of the general public. A service dogs work does not disrupt the normal course of business.
Public Appropriateness:
The dog is clean, well groomed, does not have an offensive odor and does not urinate or defecate in inappropriate locations.
Service Dog Etiquette
DONT pet, talk to, make eye contact or distract the dog in any way. DO allow the dog to work without distraction. DONT speak to the dog when greeting a service dog team, speak only to the handler. DO ask for permission to pet the dog. Under certain circumstances, the handler may permit it. DONT be insulted if your request to pet the dog is denied. DO realize that allowing the dog to greet you may distract the dog from its work. Because these are friendly dogs, they enjoy attention, however, such distraction may interrupt the dogs work and could cause injury to the dogs handler. Keep this in mind when tempted to pet or speak to a service dog
Service Dog Training
ADI (Assistant Dog International) requirements include, but are not limited to, the following: The dog be specifically trained to perform 3 or more tasks to mitigate aspects of the clients disability. Dog demonstrates basic obedience skills by responding to voice and/or hand signals for sitting, staying in place, lying down, walking in a controlled position near the handler and coming to the handler when called. Dog works calmly and quietly on harness, leash or other tether. Dog is able to perform its tasks in public. Dog must be able to lie quietly beside the handler without blocking aisles, doorways when possible. [dog trainer information links here]
LAWS
Federal laws
Americans with Disabilities Act (ADA) revised in July 2010 Federal Air Carrier Access Act of 1986. The act requires air carriers to permit service animals to accompany persons with disabilities on flights (14 CFR 382.55 (a)) Fair Housing Act of 1988 (FHA)
New Hampshire Laws
Service animals defined. (RSA 167-D:1) Service Animals and search and rescue dogs. (effective date Jan.1, 2012) Unlawful to disguise a pet dog as a service dog (RSA 466:8 II) It is unlawful to fit an animal with a collar, leash or harness of the type which represents that the animal is a service animal, or service animal tag issued under RSA 466:8 (effective date Aug. 12, 2012) Licensing of service dogs (RSA 466:8) This provides for free registration for the working life of a service dog (effective date Aug. 12, 2012). No companion/pet dogs in restaurants (RSA 466:8) A restaurant owner may allow his or her properly disciplined companion/pet dog inside his or her place of business. Such dog shall be removed from any portion of the premises where members of the public are present in the event a service animal is present. (effective date Jan. 1, 2012)
ADA Business Brief on Service Animals. A 1-page publication explaining the requirements of the ADA regarding animals that accompany and provide services for a person with a disability in businesses.
Commonly Asked Questions About Service Animals. A 3-page publication explaining the requirements of the ADA regarding animals that accompany and provide services for a person with a disability.
ADA Information for Law Enforcement, including training videos. Note: these documents are noticeably absent any references to service animals.
"Remember.Research is the key to your cure!"
Mobile Web App for Safe/Unsafe Drug List.
Thursday - July 4, 2013 @ 17:03:44
We sincerely appreciate the hard work of APF member, Mr. Nicholas Frias , who designed a fantastic Mobile Web App for the Safe/Unsafe Drug List for the Acute Porphyrias. He combined the APF list and the European and South African lists to create an easy to search list.
This Mobile Web App is very simple to use. All you need to do is enter Mobile Web App for Safe?Unsafe Drug List into your mobile device web browser to access it. Follow easy instructions to add the list to your home screen.
The desktop version works well, too. Mr. Frias will be updating the list with the assistance of porphyria expert, Dr. Peter Tishler. There is comment sections to track glitches in the system, so please feel free to add your comments, as Mr. Frias will continue to update the site.
This is a very special gift from Mr. Frias to people who have one of the acute porphyrias. Please join the APF in sending him our sincerest thanks.
"Remember.Research is the key to your cure!"
On Sound Footing The Health of Your Feet
Thursday - July 4, 2013 @ 16:56:12
On Sound Footing The Health of Your Feet
Your feet are pretty small, considering they have to support the entire height and weight of your body. But they can cause big problems. So pay some attention to your feet.
Feet dont get any respect, says Dr. Marian T. Hannan, who studies foot disorders at the Institute for Aging Research at Hebrew SeniorLife. Theyre sort of the Rodney Dangerfield of the human body.
Each step you take involves a remarkably intricate network of bones, muscles, tendons and ligaments. That complexitycombined with all the weight they carryaccounts for why feet can be so prone to problems, including bone fractures, arthritis and plantar fasciitis, a swelling of the thick band of tissue that runs along the bottom of the foot.
If left untreated, foot problems may worsen. Eventually, the pain could interfere with your ability to do even the most basic things like walking up stairs or down the street. If pain alters the way you walk, it can lead to pain in your knees, hips and back as well. These problems can multiply, limiting your activity and affecting your quality of life.
Several things can contribute to foot pain or numbness. Sports and physical activity can cause your feet to hurt or become numb. Going too far, too fast or not warming up properly before exercise can set you up for painful or numbing injuries.
Excess weight puts extra stress on your feet. Poorly fitting shoes and other footwear are common causes of foot problems as well.
Health problems can also affect the feet. Lack of feeling in your feet could be a sign of a serious illness, such as diabetes or a nerve disorder. See your health care provider if you have unusual numbness in your feet or foot pain that is severe, comes on suddenly, or doesnt improve with simple measures such as rest or over-the-counter pain medications.
The good news is that most foot disorders are either treatable or modifiable, Hannan says. The first thing that you can do is notice and keep track of it to see if theres a pattern to it. Once you figure out when you feel pain or numbness, she explains, talk to an expert who can help.
How you walk and move affects your feet. Part of that is inherited. Not only do our feet look like our parents but we also walk like our parents, Hannan says. But you can modify your gaiteither with training or by changing shoes or using shoe inserts or pads.
You can help keep your feet healthy by wearing comfortable, well-fitting shoes. Wash your feet regularly (especially between your toes), wear clean socks and try to rotate your shoes to give them time to air out.
The more you exercise your feet, the better the blood flow is to the feet, and thats important for general foot health, Hannan says.
Walking is a great way to exercise your feet. You can also try specific foot exercises. Sit down and rotate your ankles in one direction, then the other. In bare feet, sit in a chair and curl your toes, then spread them out. This helps stretch and strengthen your feet to help you balance.
Seeing what someones foot looks like is incredibly informative, Hannan says. I think were going to be seeing a lot more health care providers paying attention to the feet, she predicts.
Remember..Research is the key to your cure!"
Weighing the Evidence to Prevent On-the-Job Pain
Tuesday - July 2, 2013 @ 20:26:55
Weighing the Evidence to Prevent On-the-Job Pain
By INGFEI CHEN
It is a fact of life that job and career can be stressful. But some occupations also take a physical toll: persistent aching, throbbing or tingling in the hand, wrist, elbow, shoulder or neck.
These insidious soft-tissue ailments variously known as repetitive strain injuries, cumulative trauma disorders or work-related musculoskeletal disorders include the debilitating nerve injury of carpal tunnel syndrome and the inflamed tendons of tendinitis. They not only can cripple a persons ability to earn a living. They may also make it difficult even to twist the lid off a jar, wash the dishes or turn the steering wheel.
Therapies like steroid injections, pain relievers or surgery can go a long way in alleviating pain. But treatments do not always offer a definitive cure, and injuries can recur. Prevention is therefore paramount.
To reduce the risk of injury, many workplaces, with help from researchers, have adopted ergonomic interventions: measures that tailor equipment or job routines to accommodate the human body. But while real-world success stories abound, scientists are still sorting through the evidence to determine which ergonomic measures really work.
Each year, more than 100,000 new cases of upper-extremity ailments are reported to the Occupational Safety and Health Administration. Problems are especially common among those who do heavy or frequent manual handling and lifting tasks, whether in manufacturing, construction, meatpacking or nursing care.
But repetitive strain injuries are perhaps most infamously associated with computer use. Widespread media coverage in the late 1980s and early 90s described an emerging plague of wrist pain from carpal tunnel syndrome in computer keyboard operators, writers and other office workers.
Skepticism arose over whether tapping on a keyboard, or other more forceful repetitive motions, could result in so much discomfort and disability. In the years since, researchers have established that exerting the hands, arms or shoulders in tasks that require high levels of force, many repetitions, awkward postures or high amounts of vibration increases the risk of musculoskeletal disorders.
But research in the last decade has established that carpal tunnel syndrome is not as common in computer users as people have believed in the absence of good evidence that it was, said Dr. Fredric E. Gerr, an occupational medicine physician and ergonomics investigator at the University of Iowa in Iowa City. And whether typing actually causes that disorder remains controversial, with some recent studies calling into question any significant connection.
Nonetheless, he added, The epidemiological evidence is overwhelming that the more people type, the more pain they have.
Neck and shoulder pain is the most common upper-extremity musculoskeletal problem among computer users. In a 2002 study tracking 632 computer users newly hired at major Atlanta companies, Dr. Gerr and colleagues observed that roughly 60 percent developed neck or shoulder pain in the first year, though the study did not track how long symptoms persisted. About 40 percent reported hand or arm symptoms, mostly from tendinitis. Only 1 percent developed carpal tunnel syndrome.
Younger generations growing up in the digital age are likewise joining the ranks of the typing wounded. Surveys at two universities found that 40 to 50 percent of undergraduates experience upper-extremity pain from using their computers. Colleges do not build dormitory furniture to be ergonomically adjustable, said Dr. Benjamin Amick, scientific director of the Institute for Work and Health in Toronto, who was a co-author of those studies. They build it to be indestructible.
In the business sector, many companies have made significant ergonomic improvements to the work environment, particularly in office and manufacturing settings, experts said. The idea is to minimize the stresses on hands, arms and shoulders.
For instance, in offices since the 90s, thick keyboards with stiff keys have given way to thinner, softer-touch versions. More attention is also paid to proper positioning of the keyboard, monitor and chair and to alternative types of computer mice. And in some automobile manufacturing plants, companies have modified assembly-line equipment to take some of the physical load off workers, along with making changes to rotate employees along the line.
Employers are recognizing that you need variety in the motions that you do, rather than constantly using the same exact muscles and nerves and tendons, said Barbara Silverstein, research director at the Safety and Health Assessment and Research for Prevention program of the Washington State labor department.
Such changes often pay off. In a soon-to-be published analysis of data from more than 5,000 Washington companies surveyed in 1998, 2001 and 2003, Dr. Silverstein found that businesses that reported implementing ergonomic measures also saw a decrease in musculoskeletal injuries and absenteeism rates.
In addition, according to the federal Bureau of Labor Statistics, the number of repetitive strain cases per 10,000 full-time workers dropped from a high of 41 in 1994 to 24 in 2001. (The agency has stopped tracking data in this category of repeated trauma disorders.) However, some researchers say that the data is unreliable and undercounts all occupational injuries and illnesses, because of problems with underreporting and with changes in recordkeeping requirements.
Meanwhile, scientists are seeking to build a base of rigorous evidence for ergonomic prevention strategies to convince skeptics of their value. But so far, reviews of the research have turned up limited or conflicting proof of positive benefits from such measures as stretching exercises or various workstation adjustments for computer users.
A major difficulty is that although many studies have demonstrated ergonomic measures to be helpful, few have been the kind of large, high-quality randomized controlled trials that provide clear-cut answers, said Dr. David Rempel, an ergonomics researcher at the University of California, Berkeley. Such trials are costly and complex to design well for workplace settings, he explained, and federal financing for workplace safety studies is scarce.
A lot of us are banging our heads against that wall now, Dr. Gerr said of the challenge of ascertaining which interventions work.. In the absence of definitive evidence, clinicians continue to exercise their best judgment in finding good solutions for their patients.
An EPP Family in Texas & Australia Cathleen Mouledoux does not have EPP, but she knows the disease well because her daughter Celeste suffers from it. The disease is in Cathleens husbands family, but Rene was never troubled by it, playing outside all the time as a child without anything more than a sunburn. Rene was only tested for Erythropoietic Protoporphyria until after he and Cathleen found out their little girl had EPP. Celeste had always shown low tolerance for the sun from the time she was a baby. The first time Cathleen noticed the problem Celeste was playing outside in dappled sunlight, mostly shaded by a large tree, and suddenly started crying inconsolably. Cathleen remembers it clearly because Celeste was not a fussy child, and when Cathleen took her indoors, she saw that Celeste was browned on her nose and her cheeks, just from the short time shed spent outdoors in the shade. Celeste browned like that a few times as a child, and her skin would peel afterwards. But instead of peeling like a sunburn, the skin would come off in big chunks. As a toddler Celeste had a bad burning sensation in the skin on her hands when she was exposed to the sun. Nothing Cathleen tried eased the pain, but there were no visible symptoms. Then when Celeste was about four years old, she broke out in tiny little bumps that looked like bug bites after being out in the sun. The family called them spider eyeballs and again Celeste suffered terrible pain with sun exposure. When Celeste was 13 years old, her mother learned that two cousins had a disease called Erythropoietic Protoporphyria. Their symptoms were pretty similar to Celestesall three kids would experience dramatic swelling in their hands and faces whenever they played in the sun. Cathleen took Celeste for testing and the diagnosis was made. Not being able to tolerate outdoor activities as a child was hard on Celeste as the family moved around in the warm and beach-friendly American South. Cathleen remembers her daughter going to the beach with a group of friends one day as a teenager, going along with her friends and getting major sun exposure, and coming home bright red with her skin hugely swollen and painfulher arms were dramatically swollen all the way up to where the coverage from her t-shirt sleeves stopped and the swelling and pain took six weeks to heal completely. The one reprieve came when Renes job moved the family to Australia for several of Celeste high school years. Sun protection is a big topic in Australian public health notices because skin cancer is a major problem there. So the family found significant public awareness and acceptance of the need to cover up. Broad-brimmed hats were part of the kids school uniforms, and kids bathing suits often offered as much coverage as shortie wetsuits. Like other people with all sorts of diseases, Celeste has sometimes chafed against the restrictions imposed by her EPP. Cathleen remembers her daughter going to the beach with a group of friends as a teenager one summer day, and coming home with every exposed portion of her skin bright red, hugely swollen and painful. The swelling and pain took six weeks to heal completely. But now Celeste is a young woman in her early 20s and doing well. She knows what she needs to do to protect her skin from the sun, and she takes precautions to keep herself healthy.
Global Genes RARE Project and a host of partners are proud to continue our RARE Webinar Series, a series of educational webcasts this year on relevant and timely topics that should be of interest to the RARE community.
Our upcoming webinar will focus on Understanding Rare Disease Registries and will feature panelists coming at this topic from a different angle.
Understanding Rare Disease Registries: Gain a clear understanding of design, implementation, and resource considerations that are the foundations of a successful registry in this two-part webinar series.
Part 1, July 31, 2013 11:00 am Pacific Time Register today - space is limited!
Part one of this series will cover the different types of registries and features of a robust patient registry, as well as options currently available for building a new registry or enhancing an existing one. The expert panelists will discuss resources for questionnaire design, collecting natural history information, considerations for drug development and the FDA, and informed consent and data sharing.
Panelists for Part 1 include:
Dr. Steve Groft, Director of the Office of Rare Diseases (ORD)
Dr. Marshall Summar, Division Chief of Center for Genetic Medicine Research (CGMR)
Moderator: Shira Kramer, President, GlobalEpi Research
I would encourage you to register and join the discussion. I would also ask that you send this email along to your community and rare friends that might also be interested in the topic.
Special thank you to our content partner, GlobalEpi Research, for their help in coordinating this important discussion.
(Health.com) -- Gillian Aldrich started growing vegetables in her backyard three years ago, and she's now working on planting a bed of hydrangeas, butterfly bushes, rose campion, and -- her favorite -- pale-pink hardy geraniums along one side of her property.
As she digs in the garden, her 8-year-old daughter and 3-year-old son often play around her, sometimes taking a break to dig for worms or pick strawberries.
Instead of watching them, Aldrich is playing, too -- "my kind of play," she says.
"When you sit at a desk all day, there's something about literally putting your hands in the dirt, digging and actually creating something that's really beautiful," says Aldrich, 42, a magazine editor in Maplewood, New Jersey. "There's something about just being out there that feels kind of elemental."
Aldrich isn't the only one who feels this way. Many gardeners view their hobby as the perfect antidote to the modern world, a way of reclaiming some of the intangible things we've lost in our busy, dirt-free lives.
The sensory experience of gardening "allows people to connect to this primal state," says James Jiler, the founder and executive director of Urban GreenWorks, a Miami-based nonprofit that creates garden and park programs for low-income neighborhoods.
"A lot of people [understand] that experience. They may not be able to put it into words, but they understand what's happening."
Working in the garden has other, less spiritual rewards. In addition to being a source of fresh, healthy produce, gardening can ease stress, keep you limber, and even improve your mood.
Here are just a few of the ways gardening can benefit your physical and mental health, and how you can start harvesting those benefits for you and your family.
Stress relief
A recent study in the Netherlands suggests that gardening can fight stress even better than other relaxing leisure activities.
After completing a stressful task, two groups of people were instructed to either read indoors or garden for 30 minutes. Afterward, the group that gardened reported being in a better mood than the reading group, and they also had lower levels of the stress hormone cortisol.
"We live in a society where we're just maxing ourselves out all the time in terms of paying attention," says Andrea Faber Taylor, Ph.D., a horticulture instructor and researcher in the Landscape and Human Health Laboratory at the University of Illinois at Urbana-Champaign.
Humans have a finite capacity for the kind of directed attention required by cell phones and email and the like, Taylor says, and when that capacity gets used up we tend to become irritable, error-prone, distractible, and stressed out.
Fortunately this "attention fatigue" appears to be reversible. Following a theory first suggested by University of Michigan researchers in the 1980s, Taylor and other experts have argued that we can replenish ourselves by engaging in "involuntary attention," an effortless form of attention that we use to enjoy nature.
Trading your BlackBerry for blackberry bushes is an excellent way to fight stress and attention fatigue, Taylor says, as the rhythms of the natural environment and the repetitive, soothing nature of many gardening tasks are all sources of effortless attention.
"The breeze blows, things get dew on them, things flower; the sounds, the smells," says Taylor, herself a home gardener. "All of these draw on that form of attention."
Better mental health
The effortless attention of gardening may even help improve depression symptoms.
In a study conducted in Norway, people who had been diagnosed with depression, persistent low mood, or "bipolar II disorder" spent six hours a week growing flowers and vegetables.
After three months, half of the participants had experienced a measurable improvement in their depression symptoms. What's more, their mood continued to be better three months after the gardening program ended. The researchers suggest that the novelty of gardening may have been enough to jolt some of the participants out of their doldrums, but some experts have a much more radical explanation for how gardening might ease depression.
Christopher Lowry, Ph.D., an assistant professor of integrative physiology at the University of Colorado at Boulder, has been injecting mice with Mycobacterium vaccae, a harmless bacteria commonly found in soil, and has found that they increase the release and metabolism of serotonin in parts of the brain that control cognitive function and mood -- much like serotonin-boosting antidepressant drugs do.
Digging in the dirt isn't the same as taking Prozac, of course, but Lowry argues that because humans evolved along with M. vaccae and a host of other friendly bugs, the relative lack of these "old friends" in our current environment has thrown our immune systems out of whack.
This can lead to inflammation, which is implicated in a host of modern ills, from heart disease to diabetes to depression.
"By reintroducing these bacteria in the environment, that may help to alleviate some of these problems," Lowry says.
Exercise
Gardening gets you out in the fresh air and sunshine -- and it also gets your blood moving.
"There are lots of different movements in gardening, so you get some exercise benefits out of it as well," says William Maynard, the community garden program coordinator for the City of Sacramento's Department of Parks and Recreation.
Gardening is hardly pumping iron, and unless you're hauling wheelbarrows of dirt long distances every day, it probably won't do much for your cardiovascular fitness.
But digging, planting, weeding, and other repetitive tasks that require strength or stretching are excellent forms of low-impact exercise, especially for people who find more vigorous exercise a challenge, such as those who are older, have disabilities, or suffer from chronic pain.
As a pleasurable and goal-oriented outdoor activity, gardening has another advantage over other forms of exercise: People are more likely to stick with it and do it often.
"It's not just exercise for exercise itself, which can become tedious," says Katherine Brown, the executive director of the Southside Community Land Trust, a nonprofit that supports community gardens and other urban agriculture in and around Providence, R.I. "It's exercise that has a context, that reinforces the limberness of your limbs and the use of your hands. You've got a motivation for why you want to grip. You're not just gripping a ball, you want to pull a weed."
Brain health
Some research suggests that the physical activity associated with gardening can help lower the risk of developing dementia.
Two separate studies that followed people in their 60s and 70s for up to 16 years found, respectively, that those who gardened regularly had a 36% and 47% lower risk of dementia than non-gardeners, even when a range of other health factors were taken into account.
These findings are hardly definitive, but they suggest that the combination of physical and mental activity involved in gardening may have a positive influence on the mind.
And for people who are already experiencing mental decline, even just walking in a garden may be therapeutic. Many residential homes for people with dementia now have "wander" or "memory" gardens on their grounds, so that residents with Alzheimer's disease or other cognitive problems can walk through them without getting lost.
The sights, smells, and sounds of the garden are said to promote relaxation and reduce stress.
Nutrition
The food you grow yourself is the freshest food you can eat. And because home gardens are filled with fruits and vegetables, it's also among the healthiest food you can eat.
Not surprisingly, several studies have shown that gardeners eat more fruits and vegetables than their peers.
"People who are growing food tend to eat healthy," says Brown. "The work that we do here with kids demonstrates it on a daily basis, throughout the seasons."
Studies of after-school gardening programs suggest that kids who garden are more likely to eat fruits and vegetables. And they're a lot more adventurous about giving new foods a try, says Anne Palmer, who studies food environments as the program director of Eating for the Future, a program based at the Johns Hopkins School of Public Health Center for a Livable Future, in Baltimore.
"I've watched a lot of cooking and gardening classes with kids," Palmer says. "It's amazing how many of them will try things like radicchio or some kind of unusual green that has a pretty strong flavor, like arugula, and they'll say, 'Wow, this is good.'"
Not to mention that homegrown produce simply tastes better.
"It's incomparably more delicious to eat something that's fresh," Brown says.
How to get started
You don't need a big backyard or a green thumb to benefit from gardening. If you have very little space or experience, you can start out with just a few houseplants, or you could even try gardening in containers.
"You can grow a wonderful crop of cherry tomatoes in nothing more than a five-gallon bucket that you've cleaned really well and put holes in the bottom of," Brown says.
For novices who want to learn the basics of gardening, a huge -- and somewhat overwhelming -- variety of information is available on the Web and in bookstores. But one of the best ways to get started is to meet some other gardeners, who can be found in local garden clubs and community gardens in just about any town or city.
For some great gardening tips, just start up a conversation with one of the gardeners next time you are passing by a community garden.
"Most will love to share their gardening savvy," Brown says. "That's a really nice way to start."
Remember..Research is the key to your cure!"
Stressed? Maybe You Should Have Your Heart Checked
Friday - June 28, 2013 @ 12:03:47
Stressed? Maybe You Should Have Your Heart Checked
Those who thought pressure was affecting their health twice as likely to suffer heart attack, study says
People who think stress is affecting their health may be setting themselves up for a heart attack, a new study contends.
The researchers found that these people had double the risk of a heart attack compared with people who didn't think stress was harming their health.
"People's perceptions about the impact of stress on their health are likely to be correct," said study author Hermann Nabi, a senior research associate at the Centre for Research in Epidemiology and Population Health at INSERM in Villejuif, France.
"They may need to take actions when they feel that it is the case," he added.
These findings have both clinical and theoretical implications, Nabi said.
"From a clinical perspective, they suggest that complaints of adverse impact of stress on health should not be ignored in clinical settings as they may indicate increased risk of developing coronary heart disease," he said.
From a theoretical perspective, the findings imply that the perceived impact of stress on health is a valid concept that should be considered in future studies aimed at examining the association between stress and health outcomes, Nabi added.
The report was published June 27 in the online edition of the European Heart Journal.
Dr. Gregg Fonarow, a professor of cardiology at the University of California, Los Angeles, said that "stress and reactions to stressful situations have been associated with increased risk of cardiovascular disease in many studies."
However, few studies have looked at whether an individual's perception of stress is associated with cardiovascular outcomes, he said.
And it's not clear if reducing stress would affect the risk for heart attack, Fonarow said.
"Further studies are needed to determine whether stress reduction or other risk reduction strategies can reduce cardiovascular events in men and women who perceive they are under stress that is adversely impacting their health," he said.
For the study, Nabi's team collected data on more than 7,000 men and women who took part in the Whitehall II study, which has followed London-based civil servants since 1985.
Participants were asked how much they felt that stress or pressure in their lives had affected their health. Based on their answers, they were placed into one of three groups: "not at all," "slightly or moderately," or "a lot or extremely."
Participants were also asked about their levels of stress and other lifestyle factors such as smoking, drinking, diet and physical activity.
The researchers also collected medical information, such as blood pressure,diabetes status and weight, and other data, including marital status, age, sex, ethnicity and socioeconomic status.
Over 18 years of follow-up, there were 352 heart attacks or deaths from heart attack.
After taking all of these factors into account, the investigators found those who said their health was a "lot or extremely" affected by stress had more than double the risk of a heart attack compared with those who said stress had no effect on their health.
After further adjustments for biological, behavioral and other psychological risk factors -- including stress levels and measures of social support -- the risk wasn't as high. But it was still a lot higher (49 percent higher) than among those who said stress didn't affect their health, the researchers noted.
While the study found an association between perceived levels of stress and heart attack, it did not prove cause-and-effect.
Samantha Heller, a senior clinical nutritionist at NYU Langone Medical Center in New York City, offered some tips on dealing with stress.
The stress response is not only a mental reaction to a situation, but a physiological reaction, she explained.
"Acute and chronic stress over time can make us sick. Our perception of how that stress affects our health may be an additional stressor biochemically, psychologically and physiologically, creating a feedback loop that results in increased physical distress and disease," Heller said.
Managing stress does not mean ignoring it, she said. "Working with a qualifiedmental health professional who specializes in cognitive behavioral therapy can be very helpful. In lieu of that, there are some things you can do on your own."
·Take several slow deep breaths periodically throughout the day. Deep breathing can shift the body out of the fight-or-flight response.
·Exercise regularly. Cardiovascular exercise teaches the body how to handle the physiological effects of stress. It also helps reduce anxiety and depression.
·Eat as healthfully as possible. Chronic or acute stress may trigger the desire to dive into high-calorie comfort foods. However, after an initial flash of relief, you will tend to feel lethargic, fatigued and possibly worse than you did before.
·Identify stressful triggers, and create a plan to help you cope.
·Instead of stressing about your health, be proactive and find ways to improve it. If you have high blood pressure, learn how to lower the sodium in your diet. Start walking a few days a week to strengthen your heart and help manage weight.
Remember..Research is the key to your cure!"
UPDATE: Dr. Peter Tishler and APF Drug Database
Wednesday - June 26, 2013 @ 18:22:39
Summer, 2013
Dear American Porphyria Foundation Member:
I hope you have been using the APF Drug Database (http://APFdrugdatabase.com), which we established some years ago. I am updating the drug database once again, to add new medications and reinforce or change the safety of existent medications. Thus, I write once again to ask all APF members with an acute porphyria (intermittent acute porphyria, variegate porphyria, coproporphyria, ALA dehydratase deficiency porphyria) to provide information regarding your medications.
Please complete the attached Evaluation of Medications form for each medication, Make a second copy if you have more medications to list. Return it to the APF soon, using any of the mailing procedures listed below. This will be very helpful. I may contact you to clarify aspects of your report.
Many thanks.
Peter Tishler, MD
American Porphyria Foundation, 4900 Woodway, Suite 780, Houston Texas 77056-1837
A friend asked me to help them understand my disorder and how I live with it. Please feel free to comment. I would like your input to see if this help people understand.
Imagine that you lived in a world with ONLY peanuts All their was to eat was peanuts, you worked at a factory that processed peanuts, you grow peanuts at home to save money and there is no way to avoid peanuts 100% Now imagine your allergic to peanuts. Every time you smelled peanuts you broke into hives. Every time you touched peanuts it burned your skin like pouring hot wax on it. And God for bid you ate one..(but remember peanuts are the only food source around) it would cause uncontrollable nerve vibrations, shivering, burning, itching, swelling, scaring, and pain that is so bad your brain wont let you body sleep.
Where would you find the power to wake up every morning and go to work and provide for your family?
Where does this strength come from knowing you will be in severe pain for days, weeks or months?
How do you survive without any help from friends or family?
Life with a disorder sucks!!!!! But I guess its still a life.
I hope this helps you understand.
Victor has EPP.
In talking with Victor I really hope that those with a Disorder reach out to their families and friends. They may hear you express that your ill or not feeling well but ask yourself: Do they really understand my disorder and how it affects me daily?, Can they help me? If so how?
Sometimes some may say your crazy, stop complaining about it, get on with your life. Some may do nothing at all. But stop for a moment this disease/disorder you have your not the only one that suffers family, friends, associates everyone suffers. So be proactive with your spouse, children do what you can talk about during family time, make it a point to interact with family and friends the best you can when you can. Have a positive attitude and do your best and try.
"Remember..Research is the key to your cure!"
"Remember..Research is the key to your cure!"
What One Woman Can Do
Wednesday - June 26, 2013 @ 18:22:53
Jennie Eberhardt
Type of Porphyria:
Acute Intermittent Porphyria (AIP)
What One Woman Can Do
APF Sponsor, Jennie Eberhardt, has been awarded the 2006 APF Ambassador for the work she has done in her community. She is a one-woman porphyria awareness dynamo. Before her illness, Jennie enjoyed a successful career as a professional make-up artist with theaters and photographers. Her work took on other unusual aspects. For instance, she created mock victims to help train ambulance crews for disaster drills. She also did the make-up for cancer patients. One of her most gratifying experiences was to create a jaw line for a woman who had lost part of her jaw to throat cancer surgery. But her most enjoyable career experience was as the make-up artist for a production with female impersonators. In fact, Jennie developed such a great relationship with her clients that they are now some of her biggest supporters and encouragers since her illness. Jennies career also encompassed beauty pageants and image consulting; an active life to be suddenly halted when she developed severe chemical sensitivities. Then she was also diagnosed with AIP. But Jenny "made lemonade" out of her mound of lemons by changing from a career of sales and marketing to a "ministry" of promoting porphyria awareness and education. As a very active Sponsor of the IN TOUCH network, Jennie has provided a loving shoulder for many of our APF Sponsors.
"Remember..Research is the key to your cure!"
Ho well do you rank your sleep?
Tuesday - June 25, 2013 @ 09:49:12
I believe that 7 hours of sound sleep are the perfect amount. Now for some of us 6 may be good, 8 may be better. I have listed below how I rank every hour of sleep. Read it over and tell me if you agree, disagree or have your own ideas for ranking every hour of sleep. Enjoy!
Hour 7: Perfect ammount
Hour 6: still a good amount but you wake feeling like you dont want to get out of bed.
Hour 5: You definately did not get enough sleep but give me my mocha java and i'll be fine.
Hour 4: I have to get up after 4 hours? Okay fine but I better have my own whole pot of coffee waiting for me!!!
Hour 3: Really? Are you serious? I better have a really good reason to be getting up after 3 hrs of sleep!
Hour 2: At 2 hours of sleep why does one even try to go to sleep? I mean all it is at this point is a cruel dirty trick. Good luck haveing day thats anything above mediocre!
Hour 1: You simply dont sleep. It's like when you lay down for a nap and yet cant fall asleep. Why did you even try" you ask yourself?
Now for those times when you get to sleep over 7 hours.
Hour 8: You must have been able to sleep in. You wake up feeling totally refreshed and think yes, today will be a good day.
Hour 9: This must be a Saturday morning and you have no plans to be able to sleep this long. But its a good thing! Scooby-Doo, Looney Toons, or watching that episode of "The Office" that you DVR on thursday. Your the envy of everyone who has to work that day.
Hour 10: Am I sick to stay in bed this long!
Hope you enjoyed reading this and found it amusing. Have a wonderful week everyone!
"Remember..Research is the key to your cure!"
APF History
Monday - June 24, 2013 @ 14:54:59
APF History
The American Porphyria Foundation was formed in 1982 when Executive Director Desiree Lyon joined with another individual whose family was affected by porphyria to form a patient-run, expert-advised organization that would educate doctors and the general public about porphyria, raise funds for research, and advocate for better policy and patient care. At the time, Desiree was a very sick young woman undergoing treatment as an inpatient at the National Institutes of Health in Bethesda, MD. The physician-scientists treating her had explained that Acute Intermittent Porphyria was causing the horrible pain she felt, along with seizures and other neurological disturbances, immense swelling and rigidity of her abdomen, and other alarming and life-threatening symptoms. As so many of us do when we are first diagnosed, Desiree sought more information about her condition, written in language she or any other person without a medical degree could understand. She got permission from her doctors to walk herself and her IV pole down to the hospitals medical library every day and began reading everything she could find on porphyria. And from that simple beginning, this nearly-30 year old organization was born. One of the APFs earliest efforts was joining with other rare disease advocates to form the National Organization for Rare Disorders (NORD), and testifying before Congress in the same year in support of the Orphan Drug Act (1983). Panhematin, which remains the only specific treatment for acute porphyria available in the United States, was the first drug to be approved under the ODA. Since then, we have published materials on all the porphyrias for a patient audience; developed a comprehensive website and the educational DVD Porphyria Live; educated doctors at medical conferences, and through mailings and in-hospital seminars; helped thousands of patients in the U.S. and internationally find their way to diagnosis and treatment; served as liaison between the patient/primary care and research communities; and continually sought funds to improve research and training, diagnosis and care for the porphyrias.
"Remember..Research is the key to your cure!"
Are You Pooping Wrong?
Tuesday - June 18, 2013 @ 21:24:33
Ok! I know this not a subject anyone wants to talk about but it's a real thing that happens to us with Porphyria or not here are some suggestions I found that make going good. Enjoy!
Are You Pooping Wrong?
By worldwide standards, Americans are in the toilet on elimination practices.
Our ancestors did it. People in Asia, Africa, and some parts of Europe still do it. So how did we Westerners end up deviating from the best way to go No. 2?
Blame it on toilets as we know them. Thrones, they have been called. Turns out we should squat, not sit.
In a 2003 study, 28 healthy people volunteered to time themselves doing their business in three alternate positions: sitting on a standard toilet, sitting on a low toilet, and squatting. They not only recorded how long it took them, but also how much effort it took. Squatting, the study concluded, takes less time and effort.
"There is definitely some physiologic sense to squatting," says gastroenterologist Anish Sheth, MD, co-author of the books What's Your Poo Telling You? and What's My Pee Telling Me? "Simply put, it straightens out the colon."
When we're standing, the colon (where waste is stored) gets pushed up against the puborecatlis muscle, which keeps fecal continence until it's time to hit the bathroom. Sitting down only partially relaxes that muscle. Squatting fully relaxes it, essentially straightening out the colon. That, in turn, eases the elimination pooping process.
Experts have argued that digestive illnesses like colitis, constipation, and hemorrhoids stem from all the sitting and straining people do on the toilet. Studies have shown, for example, that the more time you spend in the bathroom, specifically reading, the more likely you are to develop hemorrhoids, or swollen blood vessels in and around the anus. Some doctors even recommend patients try squatting to deal with their colon issues.
Squatting toilets are used throughout the world today. In Asia, public restrooms might offer two stalls with Western porcelain flush toilets, and two stalls with squat toilets in which the user plants their feet over an opening in the floor and squats. "Turkish" toilets can be found elsewhere, including Japan, Russia, and France.
While Sheth doesn't now advise his patients to try squatting, "I probably should," he says. "I guess until now there wasn't a safe way."
Sheth was referring to SquattyPotty, a product released last fall that looks like a step stool. Users place their feet on it while sitting on the toilet, enabling a 35-degree angle squat.
What do you think? Will it catch on in the United States? Tell us in the comments!
"Remember..Research is the key to your cure!"
Have you joined the APF In Touch Network
Tuesday - June 18, 2013 @ 21:17:37
Join APF In Touch
Because porphyria is a rare disease (defined as affecting fewer than 200,000 sufferers in the U.S.), many newly diagnosed patients have never even heard of the condition before, let alone met someone else who suffers from it. We created the APF In Touch network to meet this need. APF membership includes access to the In Touch network, through which members can contact others around the country who are dealing with porphyria. Some members form lasting friendships via email, telephone or old-fashioned letters. Others prefer to reach out to members in their region and organize face-to-face get-togethers. If you are seeking support and fellowship, or are willing to be there for others who are dealing with porphyria, please fill out and send in the In Touch consent form to our address below. For more information on the APF In Touch network, contact Mira at the APF office: 866-APF-3635 or 713-266-9617. American Porphyria Foundation 4900 Woodway, Suite 780 Houston, TX 77056
What the In Touch network has done for me:
I want to share my experience with the In Touch network provided to us by the Foundation. I was diagnosed with AIP after 18 months of symptoms. You know the severe abdominal and back pains with fatigue and nausea. You all know the drill. The scariest part was the rarity of this disease. Every doctor tells you they're not that familiar with it, and very little was actually known about it. People look blankly at you when you try to explain how you feel. I don't have to elaborate to you all that also have it. So I decided to communicate with someone else that had this illness. This was back in 2001, the time before the wonderful website that we are so blessed with now. So I opened the newsletter and looked at the names before me. I knew that I wanted someone that also had AIP. So I closed my eyes and asked God to help me chose the right one. I opened my eyes and there she was. Lori Brown from Madison, Alabama. I am from Arkansas so she was geographically close to me. I emailed her and introduced myself to her, telling her all of my experiences so far and asked if she would like to share "war stories." She emailed back and was more than happy to do just that. So over the next 7 years Lori and I battled porphyria together. After a while Lori and I began calling each other on the telephone. Some of our conversations lasted for two hours! We discussed how the disease affected our marriages, children and our lives in general. I don't know if it was misery loves company but I can tell you she helped me so much. To have someone who understands what you are going through is great. I didn't feel alone. On October 16, 2008 Lori Brown from Madison, Alabama passed away. The battle with porphyria is over. She is free. I never got the privilege of seeing her face or giving her a hug. But she was one of my best friends. So if you are thinking about getting in touch with someone and just haven't done it yet I encourage you to find yourself a Lori too. Find several. I have others as well: Rose, Mira, Judy, Jennifer and Troy. Or attend a meeting scheduled near you. Or reach out and host one yourself. I can assure you it will be a fulfilling experience. Karen Eubanks Conway, AR
Call the APF 866-apf-3635 to join now!
"Remember..Research is the key to your cure!"
Have you called yet?
Tuesday - June 18, 2013 @ 21:12:21
Telemedicine Consultations
If you need to consult with a Porphyria specialist and are unable to do so because of the distance to a Porphyria center, you now have the opportunity to consult electronically.
A Porphyria specialist and member of the APF Scientific Advisory Board, Dr. Karl Anderson, will be consulting with Porphyria patients via a telemedicine service from the General Clinical Research Center of the University of Texas Medical Branch at Galveston.
To access this service, you need to first locate a video teleconferencing facility in your community. These facilities are often found in libraries, businesses, universities and research centers. Unfortunately, neither the APF nor Dr. Anderson can provide you with a list of facilities with teleconferencing capabilities. Next, call Dr. Karl Anderson (409) 772-4661 to arrange for an appointment and to find out what information you might need to have ready prior to the telemedicine visit.
During the teleconference, Dr. Anderson will discuss your case with you just as he would during a regular office visit. This project was funded in part by a grant from the American Porphyria Foundation.
Physician Information Kit Available
Upon request, the APF will send a comprehensive physician education packet on the acute porphyrias to physicians. It includes educational materials on the diagnosis and management of the acute porphyrias; information on biochemical and genetic testing; Panhematin treatment for the acute porphyrias; and a recent article from the Annals of Internal Medicineon diagnosis and management of the acute porphyrias. Please call our office at 713-266-9617 to order the kit.
In addition, the APF will also send information on PCT and EPP to physicians upon request. Please call our office at 713-266-9617 to order the packet.
These packets are delivered via USPS, for physicians only.
"Remember..Research is the key to your cure!"
Lots of Americans Want Health Care Via Smartphone
Monday - June 17, 2013 @ 14:43:00
Lots of Americans Want Health Care Via Smartphone
TUESDAY, June 18 (HealthDay News) -- Plenty of Americans are eager to use their mobile phones and tablet computers to better manage their health care, a new poll finds -- though the nation has a way to go before we're all consulting Dr. Smartphone.
In a Harris Interactive/HealthDay survey released Tuesday, more than one-third of respondents who are online said they were "very" or "extremely" interested in using smartphones or tablets to ask their doctors questions, make appointments or get medical test results.
Similar numbers of respondents were eager to use mobile phones and tablets for actual health-care services -- such as monitoring blood pressure or blood sugar, or even getting a diagnosis. Such phone and tablet apps are, however, either just getting off the ground or not yet on the market.
The survey results show that the demand for digital assists to health care is "strong and likely to grow," said Humphrey Taylor, chairman of The Harris Poll.
But he added that big questions remain: What types of services will consumers be able to get with their mobile devices, and when?
"The devil will surely be in the details," Taylor said, "and these are very big details."
An expert in health-care information agreed. "Right now, we're looking at a patchwork system," said Titus Schleyer, who heads the Center for Biomedical Informatics at the Regenstrief Institute, based at Indiana University-Purdue University in Indianapolis.
Companies are developing a number of apps that, along with equipment attached to your phone or tablet, can help diagnose everything from ear infections and eyediseases to irregular heartbeats and malaria. One goal is to bring better health care to remote parts of the world.
But there are already apps out there designed for the masses -- including ones to manage your blood pressure or blood sugar readings, for example. You take the reading via a monitor that plugs into your smartphone, and the app records all the information, which can then be e-mailed to your doctor or sent to your electronic health record, Schleyer said.
Of course, your doctor has to have the systems in place to do something with that information. And, Schleyer added, depending on where you live, and what health system you're in, that may or may not be the reality.
Schleyer said he has first-hand experience with the obstacles. His wife found an app that let her record and organize her blood pressure readings, only to discover that her smartphone "couldn't talk" to their health-care system's portal.
She ended up just bringing her smartphone to her doctor's visit.
"This poll shows us that the public is interested in using these apps," Schleyer said. "But the health-care system has to make it easier for them to do it."
Taylor said that in some other countries, services like these are more widely used because they are required or doctors are compensated to employ them. "But in this country," he said, "most doctors and hospitals have little or no incentives to provide them. They are unlikely to offer them until it is in their interest to do so."
Another poll finding was that, not surprisingly, younger adults are more eager to use their smartphones and tablets than older adults. Only one-quarter of people aged 65 and older were very interested in using the devices to help manage their blood pressure, for instance -- compared to 38 percent of younger people.
On one hand, Schleyer noted, older adults could stand to benefit the most from such technology, because they're more likely to have chronic health conditions and need more contact with their doctors.
On the other hand, they may simply not be as comfortable with smartphones and tablets as younger generations are, he said.
Despite the interest in tapping into smartphones and tablets for health care, some poll respondents had some misgivings. They were less inclined to want e-mail or text "reminders" toexercise,quit smoking, or takemedication, for example.
Schleyer said that may be because it's a bit like having your mom nag you electronically. Plus, many Americans are already inundated with e-mails and texts. "People may feel there's already too much digital information flying at them," he said.
Poll respondents were also worried about the security of their electronically transmitted medical information: 47 percent were "somewhat confident" it would be secure, while roughly 40 percent were "not very" or "not at all" confident.
That's a valid worry, Schleyer said. However, he also doubts that a hacker would have much interest in the blood pressure readings you're sending to your doctor. "They're probably more interested in your credit card number."
Schleyer thinks there's a lot of promise for technology to improve health care for Americans -- if, for instance, consumers can get not only test results sent to their phones, but also user-friendly information on what those results mean.
"But right now, none of this is mature yet," he said.
The poll results are based on an online survey of 2,050 Americans aged 18 and older, conducted between May 22-24.
"Remember..Research is the key to your cure!"
Running over obstacles to raise Awareness for Porphyria
Friday - June 14, 2013 @ 20:02:51
Merideth McGinleyis a new APF member but is already a very active one. Merideth says that the main goal of her fundraising event is to raise as much awareness for porphyria as possible. Merideth says, "My last visit to the hospital really opened up my eyes to how little medical professionals really know about the disease. If my fundraiser can help just one person has an easier experience with getting diagnosed then I will feel like I truly accomplished something." She goes on to say,"When I was 19 years old, I was diagnosed with Acute Intermittent Porphyria. Since being diagnosed in 2008, I have been in and out of the hospital and it has made me realize many people along with medical professionals do not know what Acute Intermittent Porphyria is or how to treat it". Read more of Merideths Bio
"I have decided to run in the Warrior Dash onAugust 3rdin order to raise money and awareness about this disease. Read more about the Warrior Dash at http://warriordash.com. All donations made on myAPF FirstGiving web page will go to the American Porphyria Foundation which is dedicated to raising awareness along with improving the health and well-being of individuals and families affected by Porphyria. All donations are greatly appreciated and can be made right through theAPF FirstGivingsite or by sending a check or card donation to the APF by calling 866.APF.3635".
FirstGiving is a web platform that the APF has provided for Fundraisers and Awareness campaigns to make it easy for you and your contributors to use for promoting your campaign and accepting donations that go directly to the APF.
New Panhematin brochure available for your physicians.
Friday - June 14, 2013 @ 20:01:46
New Panhematin brochure available for your physicians.
Panhematin
The APF has produced a new Panhematin brochure. If you would like a copy of the new brochure for your physician, please contact the APF and we will forward one to you promptly. Remember, too, that the APF will send your doctor a free comprehensive doctor packet for the acute porphyrias. Call 1.866.APF.3635 or email porphyrus@aol.com . If your physicians have questions about the administration or use of Panhematin, we will then send an instruction form or arrange a consultation with a porphyria expert if needed.
For the many patients who are taking Panhematin, please note that Recordati Rare Diseases, Inc. has purchased Panhematin from Lundbeck Pharmaceutical. Recordati Rare Diseases, Inc. has assured us that there should be no interruption in receiving the Panhematin treatment and that the product is the same as it has always been. In fact, for the next number of months, the telephone numbers and delivery services that were available through Lundbeck Pharmaceutical will remain the same, as well.
FYI For questions from healthcare professionals regarding general use and administration of Panhematin, please call Recordati Rare Diseases at 1-866-402-8520. Your call will be answered by a member of the Lundbeck staff on behalf of Recordati Rare Diseases until late 2013. Your physician or hospital pharmacy can order Panhematin through a wholesaler of their choice. Healthcare professionals can call 1-888-514-5204 to receive help with regular and emergency shipments, Monday thru Friday, 9 am to 6 pm EST. After hours and emergency orders, call 1-800-673-6723. In an emergency event, when the hospital/physician/wholesaler does not have Panhematin in stock, Recordati Rare Disease will ship directly from its Lavernge, TN distribution site via an expedited delivery service to anywhere in the U.S.usually within 12-14 hours.
During the 2013 International Porphyria Congress Patient Day meeting, Dr. Jean Charles Deybach spoke about the great benefit of early treatment with heme therapy ( Panhematin and Normosang)
<!--[if !supportLists]-->· <!--[endif]-->Decreased urinary ALA/PBG 2-3 days
<!--[if !supportLists]-->· <!--[endif]-->Mean abdominal pain duration 2-3 days
<!--[if !supportLists]-->· <!--[endif]-->No further severe neurological complications
<!--[if !supportLists]-->· <!--[endif]-->No major side effects in acute administration
<!--[if !supportLists]-->· <!--[endif]-->Safe use during pregnancy (Badminton & Deybach, 2006; Marsden & Rees, 2010)
Remember Research is the key to your cure!
Kathyrn Nelson & PCT
Friday - June 14, 2013 @ 19:54:26
Kathryn Nelson
Type of Porphyria:
Porphyria Cutanea Tarda (PCT)
My Porphyria Cutanea Tarda (PCT) experience began roughly seven years ago. At the time I was living in Irving, Texas. When lesions appeared on my face, forearms and legs, I thought that perhaps it was related to Psoriasis, an autoimmune disorder I had since I was a child. As a result, I resorted to a fairly common approach to Psoriasis which is exposure to UV rays. I spent an hour or so every afternoon in the sun, but more lesions developed and the existing ones grew in size. Repeated visits to my Dermatologist resulted in a variety of diagnoses including eczema, hives and finally a "picking" disorder which basically meant the doctor believes you are picking at your skin causing sores and infections. His primary reason for this was that the sores appeared only where I could physically reach the area, in other words, there were no lesions on my back or the backs of my legs. I pointed out that as a forty plus year old woman, I didn't think I had suddenly started to pick my skin but he was not deterred.I continued to use antibiotic ointments on the most severe patches and, as a result of other health concerns, discontinued my efforts to get a daily dose of UV rays. Over time, the lesions began to shrink but a new symptom developed. My skin darkened dramatically in areas where there were no blisters and where the blisters had healed, the skin turned white, giving the appearance of vitiligo. I was seeing a Rheumatologist for other autoimmune symptoms and he suggested I visit a dermatologist he knew who specialized in autoimmune skin disorders. He also prescribed Plaquenel to treat lupus-like symptoms tied to an undifferentiated connective tissue disorder. It was several months later when I met with Dr. Melissa Costner in Dallas. By that time, most of the lesions and blisters were healed, however, the splotchy dark patches and scarred white areas covered most of my arms, face and large portions of my legs. I described my experiences over the previous three years. Dr. Costner listened closely and then said she wanted to do some blood work. Three weeks later, I returned to her office where she explained I had a familial type of PCT. In one minute, all of the heartaches of the previous four years made sense. She listened to me, something the previous doctors failed to do. She believed me when I said I wasn't "picking" my skin and said that rather than affecting areas where I "could reach," PCT was actually affecting areas being exposed to the sun. By reducing the time I was spending in the sun due to my energy issues, I had actually started the PCT healing process.
Today I still have very dark patches on my skin and very white scars but I have few reoccurrences of PCT. I play close attention to the medications I take, particularly since I have other auto-immune disorders which require a heavy regimen of treatment. PCT was not something I had ever heard of and was honestly not my biggest health concern at the time. But finding a doctor who listened gave me a sense of empowerment that I continue rely on today in all aspects of my health and with all my doctors.
Remember..Research is the key to your cure!
Be Prepared for Your Appointments
Wednesday - June 12, 2013 @ 10:09:35
Visiting a Doctor is a commonplace experience, but seeing a physician in a Hospital, might produce white coat syndrome, higher anxiety event, therefore, be prepared for your appointment. Prior to the visit, think about your specific symptoms and write down all relevant information. Concentrate on what you want to know, your concerns etc. and create a questions list. Ask others around you for suggestions if that is helpful. When possible type your questions and print three copies: one for you, one for the doctor and one for the person who accompanies you. When typing your list, consider leaving room after each question to fill in the answers. The visit can nervousness and forgetfulness so the questions list is a very helpful tool. If at all possible don't go alone. Provide your companion with the list and ask him/her to take notes and listen. Four ears are always better than two in processing important information. Discussions with a doctor about possible Porphyria are tough to handle, so support is always helpful. Being informed is essential to your care and treatment so do your homework before your visit. This is good advice prior to any type of medical meeting to maximize your knowledge from the experience particularly when it involves a serious illness. A super website is www.ahrq.gov/apps/qb which deals with questions before, during and after the visit thus enabling you to create a comprehensive question list by following this user-friendly program. Modify the questions as they apply to your situation. This is a most valuable resource prior to your appointment. Be prepared in order to be better informed. This will help to ensure that you get the best possible care. Also please take time to visit, www.porphyriafoundation.com, for all your testing & treatment options.
Remember..Research is the key to your cure!
Thinking of joining the Clinical Studies? Read more
Wednesday - June 12, 2013 @ 10:04:02
Clinical Studies
There are two main types of clinical studies: clinical trials and observational studies. In a clinical trial, there is some form of treatment intervention. There is no intervention in an observational study, which is aimed at observing patients to better understand the long-term course of their disease. Clinical trials are used to test new treatments before they are approved for use by the FDA. This type of trial gives patients a chance to try out a new medication in its early stages. As with any experiment, the result of a trial is not known before its conclusion. Your participation could help demonstrate a terrific treatment breakthrough, or it could help scientists discover that a new treatment does not work after all. There may be some risk involved from the treatment in a clinical trial.
Participating in either a clinical trial or an observational study is a serious responsibility. Volunteering to participate could be a way to help yourself, affected family members and other patients by advancing medical and scientific knowledge of your condition. Some patients derive great satisfaction from assisting doctors in the study of their disease. Participation in a study can also mean a chance to meet a porphyria researcher in a clinical setting, and the consultation can be beneficial.
Go Green- Easing Brain Fatigue with a Walk in the Park
Wednesday - June 12, 2013 @ 09:55:06
Easing Brain Fatigue with a Walk in the Park
Scientists have known for some time that the human brains ability to stay calm and focused is limited and can be overwhelmed by the constant noise and hectic, jangling demands of city living, sometimes resulting in a condition informally known as brain fatigue.
With brain fatigue, you are easily distracted, forgetful and mentally flighty or, in other words, me.
But an innovative new study from Scotland suggests that you can ease brain fatigue simply by strolling through a leafy park.
The idea that visiting green spaces like parks or tree-filled plazas lessens stress and improves concentration is not new. Researchers have long theorized that green spaces are calming, requiring less of our so-called directed mental attention than busy, urban streets do. Instead, natural settings invoke soft fascination, a beguiling term for quiet contemplation, during which directed attention is barely called upon and the brain can reset those overstretched resources and reduce mental fatigue.
But this theory, while agreeable, has been difficult to put to the test. Previous studies have found that people who live near trees and parks have lower levels of cortisol, a stress hormone, in their saliva than those who live primarily amid concrete, and that children with attention deficits tend to concentrate and perform better on cognitive tests after walking through parks or arboretums. More directly, scientists have brought volunteers into a lab, attached electrodes to their heads and shown them photographs of natural or urban scenes, and found that the brain wave readouts show that the volunteers are more calm and meditative when they view the natural scenes.
But it had not been possible to study the brains of people while they were actually outside, moving through the city and the parks. Or it wasnt, until the recent development of a lightweight, portable version of the electroencephalogram, a technology that studies brain wave patterns.
For the new study, published this month in The British Journal of Sports Medicine, researchers at Heriot-Watt University in Edinburgh and the University of Edinburgh attached these new, portable EEGs to the scalps of 12 healthy young adults. The electrodes, hidden unobtrusively beneath an ordinary looking fabric cap, sent brain wave readings wirelessly to a laptop carried in a backpack by each volunteer.
The researchers, who had been studying the cognitive impacts of green spaces for some time, then sent each volunteer out on a short walk of about a mile and half that wound through three different sections of Edinburgh.
The first half mile or so took walkers through an older, historic shopping district, with fine, old buildings and plenty of pedestrians on the sidewalk, but only light vehicle traffic.
The walkers then moved onto a path that led through a park-like setting for another half mile.
Finally, they ended their walk strolling through a busy, commercial district, with heavy automobile traffic and concrete buildings.
The walkers had been told to move at their own speed, not to rush or dawdle. Most finished the walk in about 25 minutes.
Throughout that time, the portable EEGs on their heads continued to feed information about brain wave patterns to the laptops they carried.
Afterward, the researchers compared the read-outs, looking for wave patterns that they felt were related to measures of frustration, directed attention (which they called engagement), mental arousal and meditativeness or calm.
What they found confirmed the idea that green spaces lessen brain fatigue.
When the volunteers made their way through the urbanized, busy areas, particularly the heavily trafficked commercial district at the end of their walk, their brain wave patterns consistently showed that they were more aroused and frustrated than when they walked through the parkland, where brain-wave readings became more meditative.
While traveling through the park, the walkers were mentally quieter.
Which is not to say that they werent paying attention, said Jenny Roe, a lecturer at Heriot-Watts School of the Built Environment, who oversaw the study. Natural environments still engage the brain, she said, but the attention demanded is effortless. Its called involuntary attention in psychology. It holds our attention while at the same time allowing scope for reflection, and providing a palliative to the nonstop attentional demands of typical, city streets.
Of course, her study was small, more of a pilot study of the nifty new, portable EEG technology than a definitive examination of the cognitive effects of seeing green.
But even so, she said, the findings were consistent and strong and, from the viewpoint of those of us over-engaged in attention-hogging urban lives, valuable. The study suggests that, right about now, you should consider taking a break from work, Dr. Roe said, and going for a walk in a green space or just sitting, or even viewing green spaces from your office window. This is not unproductive lollygagging, Dr. Roe helpfully assured us. It is likely to have a restorative effect and help with attention fatigue and stress recovery.
Remember..Research is the key to your cure!
Remember take the time: Few Wash Hands Properly, Study Finds
Sunday - June 9, 2013 @ 21:33:03
Few Wash Hands Properly, Study Finds
Did you wash your hands properly after you used the toilet? Probably not, a new study suggests.
Researchers discreetly watched 3,749 people, 60 percent of them women, after they used public toilets in a Michigan college town. Over all, 10.3 percent did not wash their hands at all, and 22.8 percent used no soap. The remainder did use soap, but only 5.3 percent washed for longer than 15 seconds, soap or no soap. According to the Centers for Disease Control and Prevention, proper washing means rubbing vigorously with soap and water for at least 20 seconds.
Men did worse than women almost 15 percent of them did not wash at all, compared with 7.1 percent of women. People were more likely to wash their hands properly if there were motion-detection faucets, a clean sink or a sign encouraging the practice.
The authors acknowledge that the presence of even discreet observers could have affected behavior, probably encouraging more hand washing. The study appeared in The Journal of Environmental Health.
Forty-eight million people a year get sick from contaminated food, said the lead author, Carl P. Borchgrevink, an associate professor at Michigan State University, and the C.D.C. says 50 percent would not have gotten sick if people had washed their hands properly. Do as your mom said: Wash your hands.
Remember..Research is the key to your cure!
Young Children with EPP ask about Camp Discovery
Sunday - June 9, 2013 @ 21:29:12
For young people with chronic skin conditions, Camp Discovery offers a summer camping experience unlike any theyve had before. Every year, the American Academy of Dermatology sponsors a week of fishing, boating, swimming, water skiing, arts and crafts, and just plain fun.
Under the expert care of dermatologists and nurses, Camp Discovery offers campers the opportunity to spend a week among other young people who have similar skin conditions. Many of the counselors have skin conditions as well, and can provide support and advice to campers. Fun, friendship, and independence are on the top of everyones agenda and everyone shares in the discovery of what its like to be included.
Camp Little Pine Crosslake, Minnesota Ages 10-14 June 23-28*
Camp Reflection Carnation, Washington Ages 8-16 June 24-28*
Camp Big Trout Crosslake, Minnesota Ages 14-16 July 7-12*
Camp Dermadillo Burton, Texas Ages 9-15 August 11-16*
Camp Horizon Millville, Pennsylvania Ages 8-13 August 10-17
Camp Liberty Hebron, Connecticut Ages 8-16 August 11-17*
*staff would arrive one day early for orientation.
Remember..Research is the key to your cure!
History of Porphyria
Sunday - June 9, 2013 @ 21:22:08
History of Porphyria
A Little Bit of History
1841 The term porphyrin comes from the Greek word, porphyus, meaning reddish-purple. It was first thought that the reddish color of blood was from iron. One early scientist performed an experiment to prove that this was not the case. He washed dried blood with concentrated sulfuric acid to free the iron. He then treated it with alcohol and the resulting iron free residue took on a reddish purple color though it contained no iron compound
1844 - Gerardus Johannes Mulder determined the chemical composition of this purplish, iron free substance, which he named "hematin," He also illustrated that hematin took up oxygen.
1867 - J.L.W. Thudichum described the beautiful spectrum and fluorescence of these red porphyrins after he published his first book on the analysis of urine.
1871 - Felix Hoppe-Seyler crystallized hematin and described its spectrum. He then demonstrated that the crystalline form differed from one animal species to another. Using his own newly constructed gas pump, he found that oxygen formed a loose, dissociable compound with hemoglobin, which he called "oxyhemoglobin." He renamed the iron free hematin hematoPorphyrin.
1874 - Dr. J.H. Schultz described a case of a 33-year-old male weaver who suffered from skin sensitivity, an enlarged spleen and reddish urine since he was an infant. He called the condition pempigus leprosus. His was most likely the first description of protoporphyria. Dr. Schultz was later credited with giving the disease its name.
1880- MacMunn described a patients dark reddish urine of a patient with symptoms of an attack of acute Porphyria.
1888 Shortly after, sulphonal was introduced as a hypnotic drug, Joseph Stokvis had a patient who, after taking the drug, excreated the tell-tale dark reddish urine typical of porphyria. The elderly woman then became paralyzed and died. Stokvis deducted that the pigment in her urine was the hematoporphyrin.
1889 - B.J.Stokvis published the first case and clinical description of acute hepatic porphyria.
1890 - George Harley (1829-96) studied a 27-year-old who also excreted reddish urine and an "unusual nerve disturbance after taking sulphonal.
1898 - T.McCall Anderson described two brothers had eruptions with burning and pruitus on the sun exposed areas of their skin so severe that they lost part of their ears and nose. They exhibited dark urine.
1898 - Alfred F. Harris demonstrated that the urine of both brothers contained the hematoporphyrin group.
1906 - Dr. Max Dobrschansky described the first case of acute porphyria after a patient had a barbiturate.
1911 - H. Gunther classified the diseases of porphyria, including congenital erythropoietic porphyria (CEP), which he called congenital hepatoporphyria, the rarest porphyria.
1913 - Dr. Friedrich Meyer Betz injected himself with hematoporphyrins to determine their photodynamic impact . He subjected himself to the sun and became so photosensitized that the extremely painful photosensitive effect lasted several months. The photos of Dr. Betz taken hours after he injected himself illustrated his badly swollen face. He was unrecognizable until the swelling decreased. The-experiment is used today in dermatology text books. View these photos on the APF website.
1915 - Hans Fischer studied one of H. Gunthers patients, Mr. Petry, who had the rare type of Porphyria, CEP. Using data from Mr. Petrys case, Fischer provided significant insight into the chemistry of porphyrins. He also found that uroporphyrins and coproporphyrins were different from hematoporphyrins and subsequently suggested that the hemato prefix be dropped.
1923 - A. E. Garrod credits H. Gunther with first recognizing that hematoporphyria was, in fact, an inherited metabolic problem in his manuscript, Inborn Errors of Metabolism. This is the first time the term "inborn errors" of metabolism had been ever used for a group of inherited metabolic disorders and the year CEP was first identified.
1937 Dr. Jan G. Waldenstrom suggested that the name of the diseases of porphyrin metablolism be porphyrias rather than Hematoporphyrias. Using Paul Ehrlichs aldehyde reagent, Waldenstorm identified 103 patients with acute porphyria by testing their urine and noting the red color. He discovered that asymptomatic family members of these patients also had the same reaction if they ingested even small amounts of barbiturates and sulphonal. 1949 -Dr. Cecil J. Watson identified cases in which there were excessive amounts of coproporphyrins in the stool and urine and suggested that this was caused by an inborn error of metabolism. He continued his research in the United States, where he and Dr. Samuel Schwartz discovered a fundamental test, , the "Watson-Schwartz tests".
1954 - R. Schmid, Samuel Schwartz and Cecil. J. Watson classified the porphyrias according to the porphyrin content in the bone marrow and liver.
1955 - A. Goldberg and H. Berger showed that individuals with an excess of coproporphyrin had another inherited form of porphyria that they called hereditary coproporphyria. HCP is an autosomal dominant form of hepatic porphyria that is very similar to acute intermittent porphyria, except that some patients develop skin photosensitivity, too.
1960's Earnest Porphyria research in Europe and US.
1961 - Heinrich Gustav Magnus described erythropoietic protoporphyria (EPP) as a genetic disorder arising from impaired activity of ferrochelatase, which is what adds iron to protoporphyrin to form heme.
1970-2011 - Drs. Anderson, Desnick, Bissell, Bloomer, Bonkovsky,, Bottomley, Dailey, Galbraith, ,Kappas, Kreimer-Birnbaum, Kushner, Lamon, Levere, Levine, Mathews-Roth, McDonaugh, Nichols, Peters, Sinclair, Pimstone, Pierach, Poh-Fitzpatrick, Sassa, Shedlofsky, Schmid, Sassa, Tishler, Tschudy, Watson,, Phillips and many others too numerous to name have furthered porphyria research and have bettered the health care of all of us with Porphyria. We owe all these people a great debt and a great measure of thanks.
2008-2011- The APF Protect the Future program to train the next generation of experts was initiated. We are grateful for the newest experts; Drs. Manisha Balwani, Lawrence Lui, Gagen Sood, Manish Thapar, Bradley Freilich, Charles Lourenco, Brenden McGuire, Bruce Wang, Majid Rizk, Guiherme Perini, Jennifer Guy, Jeffery Wickliffe,, Aswani Singal, Sajid Mittal,Charles Parker.
King George III and Porphyria
Some historians have speculated that King George III of England suffered from Variegate Porphyria. According to notes made by the physicians attending him at that time, he suffered symptoms similar to those seen in an acute attack of porphyria: abdominal pain, constipation, rashes, confusion and severe weakness in his limbs. They also mentioned that he had dark reddish urine during these sieges and that he was often "mad." The royal physicians were not permitted to conduct extensive physical examinations, so they had to depend on what King George told them about his condition.
On one occasion when he was having a relapse of his mental and physical symptoms, Parliament debated his ability to maintain his position as King. Interestingly, he spontaneously recovered. Since George III ruled during the American Revolution, he was thought to have had a significant impact on Britian's loss to the revolutionaries. His mental and physical lapses were blamed for much of the mishandling of the war. In 1811, George suffered a severe relapse and subsequently was dethroned by the Prince of Wales.
After researching the physicians' reports, Drs. Ida Macalpine and Richard Hunter proposed that King George might have had one of the acute porphyrias. They published their theory in the British Medical Journal in 1966 and later wrote a book, George III and the Mad Business, which presented more detailed accounts of King George's malady. It is important to note that a number of Porphyria specialists and other physicians disagree with their theory. However, over the years it has been widely publicized.
Porphyria in Turkey
In southeastern Turkey, between 1956 and 1961, there were reports of an epidemic of PCT. Apparently, in 1954 the Turkish government distributed a supply of wheat seed that had been treated with fungicides containing 10% hexachlorobenzene (HCB). The wheat was originally intended for planting, but the shipment arrived too late in the season. Because there was a limited food supply in the Turkish provinces of Dijarbakir, Mardin, and Urfa, the seed was diverted for food production. It was difficult to quantify the extent and duration of HCB exposure from existing surveys, because the HCB-treated seed appeared no different from untreated supplies.
As many as 5000 individuals were reported to have been affected by the HCB treated seeds. They exhibited PCT-like syndromes as early as 1956. The government discontinued using the HCB-containing fungicide in 1959, but it was not until around 1961 that the PCT outbreak waned. Researchers from clinics near the area began to trace the dietary histories of the affected individuals and discovered that HCB appeared to be the cause of the acquired form of PCT.
Prior to this time, acquired Porphyria associated with exposure to environmental toxins was observed in experimental animal models but only rarely in humans. Shortly after the reports from Turkey were published, the association between the chronic administration of HCB to induce excessive porphyrin accumulation was confirmed in animal models as well.
Although quantitative reports of HCB exposure from Turkey are incomplete, some accounts estimate that the amount of HCB ingested by the affected individuals ranged from 0.05 to 0.2 g/d over an unknown, but "relatively long period," before changes in their skin became evident. Long-term follow-up studies by Drs. Cripp and Peters and their colleagues at the University of Wisconsin indicated that the average lag time between HCB ingestion and clinical manifestation of disease was about six months. Furthermore, their study indicated that the levels of excreted porphyrins did not correlate with the individual's age at exposure, sex, serum HCB levels, or severity of initial symptoms.
No one looks forward to a hospital stay but it doesn't have to be miserable and awful. There are some things you can do to make yourself feel more at home.
1.1
If this is a planned hospital admission get your bag packed and ready beforehand. If this is an emergency admission then have a family member bring you essential items as soon as possible.
2.2
Don't forget to bring in your medication bottles, prescription and over the counter both. Most hospital require this to get an accurate medication listing of what you are currently taking. Do not send your medication bottles home until your admission interview is completed after being assigned a room on a unit as it is needed not just for planned admissions, but emergency admissions as well. Yes, they will get a listing in the Emergency room, but the unit you are admitted to also has to see these medications, and if you have already sent them home or to the car, someone will have to bring them back in for you. If you do not have anyone with you to take these medications home, they can be locked up in a secured cabinet on the unit for you until discharge home or a family member comes in
3.3
Bring your own pillow. There is no place like home and no bed like your own but bringing your own pillow to the hospital will help you get a better night's sleep. If you have any soft comfy throw or blanket this is a plus too. Hospital linens can be stiff, rough and uncomfortable.
4.4
Bring a sweat proof thermos or large drinking glass with a lid. Nurses and staff can be very busy with the patient load they are taking care of so they may not always get that cup of ice or pitcher of water for you in a timely manner. Be prepared with your own large drinking thermos/mug. Also if you have anything in particular you like to drink such as soda, stash some of those in your room, but only if you are allowed to drink them.
5.5
Bring books, computer, cell phone etc. so you can better keep in touch with your friends and loved ones. Nothing worse than being stuck in a hospital room with no contact with your friends and family. After all you can only watch so much TV without being bored to death. Don't forget your charger or AC adapters. *Remember to make sure these items are listed as being with you in the interview chart, especially cell phones and computer notebooks.* Sometimes things have a way of walking off or disappearing before you are discharged home.
6.6
Snacks.now don't stock pile your room with tons of food. Nurses hate it when it looks like you have stockpiled your room with enough food and snacks to stay for 6 months. Have on hand some crackers or fruit, a few things to tide you over in case you get hungry in the evening or in between meals, but adhere to the diet your doctor has prescribed for you. It's a big no no to be sneaking in all kinds of junk food when you are on a diabetic or cardiac diet.
7.7
Bring music. If you are a music person, nothing is more soothing and relaxing than to put your headphones in and close your eyes and relax. If you have an mp3 player or small radio bring it loaded with your favorite music, but again make sure it is noted on the chart that you have this equipment with you.
8.8
Bring toiletries: body wash, tooth paste, comb, brush, shampoo, powder. Sure the hospital has soap, toothpaste, comb and toothbrush but these are such cheapo poor quality products. You will feel so much better using your own freshly smelling great products. Nothing makes you feel better when you are sick than getting a good shower/cleaning and smelling fresh.
9.9
Pack a robe. No one wants their rear end shining when you go for a walk down the hall and sometimes you can't always wear your own comfy pajamas, especially if you have tubes, lines, and heart monitor on. Bring slippers or easy to slip on shoes. Some hospitals have non slip socks but these are one size fits hardly any one. It would be best not to walk on the hospital floors barefoot, as they can be quite germy.
10.10
Have a pad or notebook so you can write down any questions you have for doctors. They usually come flying in, speak fast and exit fast so be ready with any questions you may have, they don't like to linger around waiting for you to think of something you need to ask. There are the few that have that great bedside manner that make you feel like you are their only patient, but these are few and far between.
11.11
Use your call bell wisely. When your nurse comes in, ask her for anything you might need/want. It is not time wise for them when they go to a patient's room and spend 15 or 20 minutes in there and ask if there is anything else they need, then walk out of the room and 2 minutes later the same patient is calling out for something. Remember shift change. At most hospitals, shift change occurs around 630 to 730 am and pm. When you call out during this time it is not likely your needs are going to be met quickly because they are trying to give/get report on patients. Seems like everyone has to go to the bathroom or need pain medicine at this time, so try to do these things before or after this time, especially when usually things people call out for during this time are not an emergency or urgent matters.
12.12
Appreciate your caregivers. Nothing makes their work so enjoyable as a simple "thank you" from their patients/family members. Everyone likes to know that they are appreciated and not many people understand how much nurses give, emotionally and physically, every day to their patients. Make a note of the names of staff that seem to go out of their way to make you feel important, and well cared for, and comment this on the surveys sent to you in the mail seeking your comments about your stay at their facility
13.13
Hospital staff is required to check on patient's wellbeing every 1-2hrs daily & nightly while you are in the hospital. If you do not want to be disturbed when you are trying to rest or sleep, please make mention of this to the nursing staff caring for you during you stay. Remember..Research is the key to your cure!
The Porphyria Consortium, APF, Protect the Future Conference
Wednesday - June 5, 2013 @ 20:11:29
The Porphyria Consortium, APF, and the Protect the Future doctors gathered in Lucerne Switzerland to attend the 2013 International Porphyria and Porphyrins Conference. The photo below is of many of the esteemed group of scientists/researchers and clinicians.
Left to Right:Howe, Makuda, Yaziki, Naik, Thapar, Marcero, Lyon, Ludke, Balwani, Latimer, Gou, Caballes, Bloomer, Singal, Bonkovsky, Perini, Bloomer, Mittal, Anderson
The next meeting in 2015 will be in Dusseldorf, Germany. Hopefully, more of you will be able to attend the outstanding Patient Day gathering, too.
We are all grateful to this group of physicians, both the present experts and the next generation of experts. When your own physicians need information about your porphyria, they look to the major medical textbooks and journal articles that the experts have written.
We are grateful; too, for the research they are performing and encourage you to find out more about the research. You have the opportunity now to participate in important research projects, which only require your time and a few tests.
Please call the APF for information. 1.866.APF.3635.
Remember..Research is the key to your cure!
Connecting Rare Disease Patients Globally a great resource!
Learn what it's like to live with a rare disease or share your own story. Browse patient testimonies, share photos, and contact patient organizations. The Understand section of RareConnect promotes awareness and understanding through daily life experiences.
Meet
Start your global conversation here. Connect with others around the world to share support and encouragement. The Meet section of RareConnect provides a safe place to meet friends, ask questions, start or join conversations, and interact with others experiencing the same challenges.
Learn
Find quality information from trusted sources. Read publications from medical experts and patient organizations. The Learn section of RareConnect links to FAQs, published articles, upcoming events, and other documents providing the latest information for each disease-specific community.
Remember.Research is the key to your cure!
Join this wonderful community for free today! If you have questions please contact Amy Chapman on FB American Porphyria Foundation.
Are you looking for additional Medical Information APF approved!
Please take a moment to research this information and incorporate into your medical information for your Doctors, they are sure to appreciate this information as great resources.
Remember.Research is the key to your cure!
A poem about Life!
Tuesday - June 4, 2013 @ 14:04:00
Life is a lot of work. What is it that gives us the strength to continue when we are tired and burned out? Sometimes an inspirational idea can help us renew ourselves and be filled with strength to fulfill our life's purpose. Inspiration comes in many forms. However, the root of all inspiration is the idea that our lives are meaningful. Inspiration is knowing that what I do matters deeply to the universe. When you have the feeling that your actions are meaningful, you will become filled with strength and vigor to fulfill your life's purpose. Remember.Research is the key to your cure!
My Life with AIP by Charles Johnson
Tuesday - June 4, 2013 @ 11:02:56
Charles Johnson
Type of Porphyria:
Acute Intermittent Porphyria (AIP)
My name is Charles Preuss Johnson and I have Acute Intermittent Porphyria (AIP). I was named after my maternal grandfather, Charles Preuss, who came to the U.S. from Germany and who died at age 39 after several bouts of severe abdominal pain. They removed his appendix, and he still had acute pain. His daughter, my mother Lorraine Preuss, died at age 49 after nine weeks hospitalized from symptoms of AIP. She suffered her whole life never knowing that her acute abdominal pain had a diagnosis of porphyria. She was a mere 67 pounds when she was finally diagnosed and that was only a few days before she died. One Saturday morning nine years ago, I awakened with agonizing pain so severe that I drove to the emergency room immediately. After a few trips to the ER and many x-rays of my abdomen, I was released with a few pills for the pain. But I continued to suffer indescribable leg pain, abdominal pain and migraines, so I went to the ER at Massachusetts General Hospital, where my mother had died. After a few hours they infused me with a liter bag of dextrose, and the pain subsided. But the urine collection that they had started when I arrived at the ER was darkening by the minute. After a few of these attacks, I was diagnosed. It was shortly after my daughter was born. Fortunately , I found a porphyria specialist at the Univ of Mass Medical Center in Worcester, MA. His name is Dr. Herbert Bonkovsky, and he was my first life saver. ( Dr. Bonkovsky is no longer at Mass General; he is a long-serving member of the APF Scientific Advisory Board) I spent a few years under his care and had my first Panhematin treatment. Dr. Bonkovsky educated my wife, Judy, and me on the triggers and dangers of AIP. When Dr. Bonkovsky took a new position in Connecticut, I switched hospitals to locate a primary care doctor in Brighton, MA . Dr. Bonkovsky continued to assist as the expert consultant. My primary care physician is also now a life saver and friend. I have been with him through so many attacks that I have lost count. He has learned a great deal through my travails with AIP. For a few years, I was admitted every six to eight weeks with acute attacks. My blood pressure would be dangerously high from the attack and I would have a number of symptoms that were difficult to manage: terrible migraines, changes in my sense of smell and taste all during the attack and sometimes afterwards. To stop the attacks before they became life threatening or lengthy, he prescribed Panheamtin. Although this helped with the attacks, it did not stop them. Only weeks later, the attack would return. I became a patient of the hospital's Pain Management Center under the care of pain doctor, who has been a tremendous support for my pain management. Porphyria patients are questioned about the need and amount of pain medication required to control an attack. He knows and understands my pain and educates others when I am admitted into the hospital. I see him every month at the clinic. I became an outpatient at the Hematology Clinic as well, and I have a hematologist there. I had an idea that maybe if I took a dose of Panhematin every two weeks on an outpatient basis, we could not just control the attakcs, but keep them from occuring. I consulted with Dr.Bonkovsky about this and he thought it was a good idea, as did my PCP and hematologist. I began the new regimen of Panhematin every two weeks. My health changed dramatically. After years of frequent admissions, I was admitted only three times in 2006. Although my first admission was for thirty days, the other two were a typical 7-8 days. This was a far cry from the previous consistent hospitalizations I had been enduring prior to the Panhemaitn every two weeks regimen. Since St. Elizabeths is a teaching hospital, I have been interviewed by many doctors and students. I have told them the same thing about the pain that Desiree said in her book: it is like "a thousand flaming swords" imbedded in my abdomen. They said this was a very understandable description and that it helps to realize the depth of porphyria pain. The nurses have been so careful and caring, too. I hope that my experience will help educate enough medical professionals so that someone else will be diagnosed correctly and treated for the acute pain without doctors doubting the level of their pain. I am a barber, and I co-owned a great shop for many years until I had to leave after the frequency of the attacks rendered me unable to keep a schedule and the pain left me unable to work. Now that I am on Panhematin every two weeks and the attacks have been under control, I am hopeful that I can return to work soon. I have four childrenthree boys and one girl. AIP is genetic, so I pray for the safety of my children. There are so many people out there that have not yet been diagnosed or have been misdiagnosed. Education on the triggers of AIP is so important. My kids may not have the mutant gene or if they do, they may never have an attack. Diet and chemical avoidance are vital to keeping the attacks at bay. I still have a good life. There are so many caring people in the world. My family, friends and neighbors have been so helpful and understanding. My wife, Judy, is my rock. She is always smiling, loving , caring. Without her, I could not have made it. I have missed many holidays and sporting events for my kids, and I cannot predict when I can go somewhere. But my mind is always busy, my phone is always ringing and I am blessed to be healthy in every other way but AIP.
Remember.Research is the key to your cure!
HOW TO DESCRIBE YOUR PAIN TO A HEALTHCARE PROFESSIONAL
Tuesday - June 4, 2013 @ 14:04:41
HOW TO DESCRIBE YOUR PAIN TO A HEALTHCARE PROFESSIONAL
1. What does the pain feel like? Circle
Aching
Agonizing
Beating
Burning
Cramping
Crushing
Cutting
Drilling
Dull
Electric
Flashing
Freezing
Gnawing
Hurting
Intense
Itchy
Jumping
Nagging
Numb
Penetrating
Piercing
Pinching
Pounding
Pressing
Pricking
Pulling
Pulsing
Quivering
Radiating
Rasping
Scalding
Searing
Sharp
Shooting
Sore
Splitting
Spreading
Squeezing
Stabbing
Stinging
Tearing
Tender
Throbbing
Tight
Tingling
Tugging
Vicious
Wrenching
2. Where does it hurt? Describe your pain- Draw it!
3. Does the pain move? Where does it travel? Does it come and go?
4. Does the pain interrupt your sleep? Do you wake up in the night or in the morning with pain?
5. What is worst and best pain levels recently? ( 1-10 Comparative Pain Scale)
1-10 COMPARATIVE PAIN SCALE
Minor- Does not interfere with most activities. Able to adapt to pain psychologically and with medication or devices such as cushions.
0 = No pain. Feeling perfectly normal.
1 = Very Mild Very light barely noticeable pain, like a mosquito bite or a poison ivy itch. Most of the time you never think about the pain.
2 = Discomforting Minor pain, like lightly pinching the fold of skin between the thumb and first finger with the other hand, using the fingernails. Note that people react differently to this self-test.
3 = Tolerable Very noticeable pain, like an accidental cut, or a doctor giving you an injection. The pain is not so strong that you cannot get used to it. Eventually, most of the time you don't notice the pain. You have adapted to it.
Moderate - Interferes with many activities. Requires lifestyle changes but patient remains independent. Unable to adapt to pain.
4 = Distressing Strong, deep pain, like an minor trauma to part of the body, such as stubbing your toe real hard. So strong you notice the pain all the time and cannot completely adapt.
5 = Very Distressing Strong, deep, piercing pain, such as a sprained ankle or mild back pain. You notice the pain all the time, and are now so preoccupied with managing causing normal lifestyle to be curtailed.
6 = Intense Strong, deep, piercing pain so strong it seems to partially dominate your senses, causing you to think somewhat unclearly. You begin to have trouble holding a job or maintaining normal social relationships.
Severe - Unable to engage in normal activities. Patient is disabled and unable to function independently.
7 = Very Intense Same as 6 except the pain completely dominates your senses, causing you to think unclearly ½ the time. At this point you are effectively disabled and frequently cannot live alone.
8 = Utterly Horrible Pain so intense you can no longer think clearly at all, and have often undergone severe personality change if the pain has been present for a long time.
9 = Excruciating Unbearable pain so intense you cannot tolerate it and demand pain killers or surgery, no matter what the side effects or risk.
10 = Unimaginable Unspeakable pain
You can print this out and take with you each time you go to the Doctor have it filled out in advance this helps doctors to ask more questions about your pain and discomfort. A handy worksheet!
Remember.Research is the key to your cure!
We need your Story for the American Porphyria Foundation~ Member Stories Section
Sunday - June 2, 2013 @ 22:36:21
Member Stories
Because Porphyria is so rare, many newly diagnosed patients have never even heard of the condition before, let alone met someone else who suffers from it. The same is true for members of the general public, and this lack of understanding in others can make life much more difficult for people living with porphyria.
We post these stories on our website to help readers connect a name and a life story with the disease. The stories here are personal they are an attempt to describe what life is like with a rare and complicated disease. To learn more about the typical symptoms and course of the disease, please see the About Porphyria section of our website.
We hope that these stories will also contribute to general awareness of porphyria, and that this will help more people to be diagnosed promptly and accurately. We thank our members for sharing some of the most intimate details of their lives with others.
We are in need of your stories. Can you be involved? Its not hard when I wrote mine, I felt very encouraged knowing that others feel the same discomfort, pain the ups and downs of Porphyria, but after reading everyones stories I was very encouraged knowing I was not alone. So please take some time to think about your story and what it means to you and how we can learn about you. IF you would like to send in your story please contact the APF by calling 1-866-apf-3635.
Remember.Research is the key to your cure!
Read about sweet Rebekah Jones and her battle with EPP
Sunday - June 2, 2013 @ 22:32:10
Rebekah Jones
Type of Porphyria:
Erythropoietic Protoporphyria (EPP)
My daughter Rebekah has Erythropoietic Protoporphyria. We live in the Grand Rapids, MI area. Rebekah was about 13 months old when she first started having symptoms. We were staying at a summer cottage on Lake Michigan. I put sunscreen on her and we went outside to play in the sand and swim. Late that afternoon she got real fussy, and by evening she was screaming and crying. We thought she was overly tired and gave her some Motrin, but she didn't sleep at all that night. In the morning, Rebekah's face and hands were swollen and red. We could not make out the bridge of her nose because of the swelling and she couldn't open her eyes or move her fingers. I called Rebekah's pediatrician and he wanted to see her right away. At first, her doctor thought she was having a reaction to the sunscreen I had used, so we tried another kind and went back to the beach! Again, Rebekah started screaming and crying, and we tried everything to calm her down. After several weeks and trips to the pediatrician with no answers, we asked to be referred to a dermatologist. She took one look at Rebekah and knew-Dr. Patel had seen a case of EPP during her residency training-how lucky for us! After the blood work came back, Dr. Patel explained what EPP was, started Rebekah on Lumitene and found the American Porphyria Foundation for us to join. Rebekah is now 10 years old and deals with her EPP very well. Usually in the spring she gets frustrated, wanting to be "normal" so she can be outside with her friends and go on school field trips. She usually helps in the school library or office instead of going outside at recess. Fortunately, the children at her school are very supportive and protective of Rebekah-the other kids even tell me when I help out at the school if Rebekah has been outside without here hat or without sun screen. Because Rebekah didn't remember her first bout of EPP, she wanted to see if it would happen again, so we let her go out for a very short period of time. That evening the burning started, her hands and face turned red and puffy and she was in a great deal of pain. Now she understands the seriousness of her condition. We have learned what works to protect Rebekah by trial and error. Even if the sun isn't out, rays can still come through-when sitting in the shade while going fishing, the sun reflects off the water, and in the winter it reflects off the snow-not a good thing! Riding in the car without tinted windows or sitting in the house in the sun light can also cause Rebekah's EPP to flare up. We have shared educational material and the APF DVD with our physician and the clinical staff, and with our family. The APF has been a great resource and support for us. Jan and Bill Jones Byron Center, MI
I lived right down the street from this family! Amy Chapman
How does one get porphyria? Most porphyrias are inherited. However, one type, Porphyria Cutanea Tarda (PCT), may either be inherited (also referred to as familial) or sporadic due to various environmental factors. In each type of porphyria there is a deficiency of a specific enzyme. These enzymes are involved in the synthesis of heme, a substance important to many body functions and are found in large amounts in bone marrow and red blood cells (which contain hemoglobin), and also has an important function in the liver and muscles. The type of porphyria present is determined by which enzyme is deficient; these enzyme deficiencies are usually inherited. Environmental factors, such as drugs, chemicals, diet, and sun exposure can, depending on the type of porphyria, greatly influence the severity of symptoms.
How are the porphyrias inherited? Can my children inherit porphyria from me? The inherited porphyrias are either autosomal dominant (inherited from one parent), autosomal recessive (inherited from both parents), or X-linked (the gene is located on the X-chromosome). Autosomal genes always occur in pairs, with one inherited from each parent. Individuals with an autosomal dominant form of porphyria have one non-working gene paired with a working (or normal) gene. Each of their children has a 50% chance of inheriting the non-working gene. Some of those who inherit the non-working gene will develop symptoms. Individuals with an autosomal recessive type of porphyria have a pair of non-working genes, and each of their children will inherit one non-working gene for that porphyria which will be paired with the working gene of their partner. Such individuals are referred to as carriers and will not have any symptoms. If two carriers of the same autosomal recessive porphyria have children, each child will have a 25% of inheriting a non-working gene from each carrier parent, and having the disorder. Because all porphyrias are uncommon, it is very unlikely that more than one type of porphyria will occur in the same family, or that a person with one type of porphyria will go on to develop another type. However, patients with more than one type of porphyria have been reported.
How are the porphyrias classified? The best way to classify a case of porphyria is to determine which enzyme is deficient, or not functioning properly. Normally these enzymes act in a sequence to make heme from simpler molecules. Heme is a vital substance for all body organs and consists of an iron atom surrounded by a porphyrin molecule. If a specific enzyme is not made properly or there is not enough of the enzyme, it cannot function properly and that step in the heme-making process cannot proceed.
Sometimes other classifications are useful. Most commonly the porphyrias are divided into the acute and cutaneous porphyrias, depending on the primary symptoms. The acute porphyrias [Acute Intermittent Porphyria (AIP), Hereditary Coproporphyria (HCP), Variegate Porphyria (VP), and ALA-dehydratase Deficiency Porphyria (ALD)] present with sudden attacks of severe stomach pain that last for several days; VP and HCP may also have skin symptoms. The cutaneous porphyrias present with blistering and scarring of the skin, pain, and/or redness and swelling in sun-exposed areas. The porphyrias may also be classified as hepatic or erythropoietic, depending on the organ where the porphyrins accumulate, the liver for the hepatic porphyrias [AIP, HCP, VP, Porphyria Cutanea Tarda (PCT), and Hepatoerythropoietic Porphyria (HEP)] or the bone marrow for the erythropoietic porphyrias [Congenital Erythropoietic Porphyria (CEP), Erythropoietic Protoporphyria (EPP), and X-Linked Protoporphyria (XLP)].
What treatment and prevention are available? To date, there is no cure for any of the porphyrias. Treatment and prevention depends on the type of porphyria. Preventive measures, which include avoidance of certain drugs and alcohol, as in the hepatic porphyrias, and sun exposure, as in the erythropoietic porphyrias, are also important in those individuals who are identified as having inherited porphyria, even if they have never had symptoms. For the acute porphyrias, hospitalization is often necessary for acute attacks. Medications for pain, nausea and vomiting, and close observation are generally required with monitoring of salt and water balance. Harmful drugs should be stopped. Attacks are treated with either glucose loading or intravenous administration of hemin (Panhematin). Attacks can be prevented in many cases by avoiding harmful drugs and adverse dietary practices.
PCT, both familial and sporadic, can be treated with regularly scheduled phlebotomies (removal of blood) to lower the amount of in the liver or a low dose regimen of hydroxychloroquine as well as removal of factors (for example, certain medications) that activated the disease.
Treatment of the cutaneous porphyrias is dependant on the specific porphyria. For CEP, blood transfusions to correct anemia, splenectomy (removal of the spleen) are often needed treatments. Bone marrow transplant (BMT) has also been done in severe cases with good results. For EPP, treatment with pharmaceutical grade β-carotene (Lumitene, Tishcon) or cysteine may improve sunlight tolerance. Avoidance of sunlight (and fluorescent lights for CEP) is recommended for all individuals with a cutaneous porphyria as well as those diagnosed with HCP or VP who have porphyria-related sun sensitivity.
Is porphyria progressive or lethal? Unlike some genetic disorders in which all individuals who inherit a gene mutation become ill,the severity of porphyria varies considerably. Such variability is due to certain additional factors other than the gene itself. Consequently, risks of severe medical difficulties or even death in the acute porphyrias are often diminished when affected individuals are well informed of their diagnosis and adopt suggested precautionary measures. Even with modern treatment and prevention, some patients still have repeated attacks. However, progressive deterioration and death from paralysis in the acute porphyrias are very unusual.
Should doctors be informed that an individual has porphyria, even if it is latent? Yes! The diagnosis of porphyria is always an important item of medical information, even when there are no symptoms. It may, for example, influence the choice of drugs to treat other conditions, the choice of anesthesia for surgery, or dietary recommendations.
What diagnostic tests are available? There are many laboratory tests available for the porphyrias, and it is often difficult to decide which should be chosen. Many of these tests are expensive. The results are often difficult to interpret. The tests vary in sensitivity and specificity. If a test is sensitive, it is unlikely to be falsely negative (that is, fail to diagnose porphyria in a patient who has the disorder). If a test is specific, it is unlikely to be falsely positive (that is, diagnose porphyria in a patient who does not have the disorder). Certain tests are both sensitive and specific in patients who have symptoms that are suggestive of a porphyria. It is advisable to have the testing performed by a laboratory that has expertise in the clinical aspects of porphyria and can provide a valid interpretation of the test results. If testing has been performed in laboratories other than porphyria laboratories, consultation with a porphyria expert is advised before a final diagnosis is made.
When abdominal and neurological symptoms suggest an acute porphyria, the best screening tests are urinary aminolevulinic acid (ALA) and porphobilinogen (PBG). When there are cutaneous symptoms that suggest porphyria, the best screening test is a plasma porphyrin assay. If one of these screening tests is abnormal, more extensive testing, including urinary, fecal, and red blood cell porphyrins, are often indicated. Urinary, fecal, and red blood cell porphyrin measurements are not very useful for initial screening because they lack either sensitivity or specificity and, therefore, are often difficult to interpret. Measurement of heme biosynthetic enzymes in red blood cells or lymphocytes is not appropriate for screening unless it is part of a family study that is done after someone in the family is already known to have a specific enzyme deficiency.
DNA testing to identify the specific mutation in an individuals porphyria-causing gene may be indicated to confirm the diagnosis of a specific porphyria. Before requesting DNA testing, it is recommended that patients have biochemical testing (urinary, stool and/or plasma porphyrins and porphyrin precursors (ALA and PBG) and/or enzyme assays). However, many patients have not had an acute attack or are not symptomatic at present, so biochemical testing may be inconclusive.
In contrast, DNA testing is the most accurate and reliable method for determining if a person has a specific porphyria and is considered the "gold standard" for the diagnosis of genetic disorders. If a mutation (or change) in the DNA sequence is found in a specific Porphyria-causing gene, the diagnosis of that Porphyria is confirmed. DNA analysis will detect more than 97% of known disease-causing mutations. DNA testing can be performed whether the patient is symptomatic or not. Once a mutation has been identified, DNA analysis can then be performed on other family members to determine if they have inherited that Porphyria, thus allowing identification of individuals who can be counseled about appropriate management in order to avoid or minimize disease complications.
What is latent porphyria? If my doctor told me that I have latent porphyria, does this mean that I will never have any symptoms? Individuals with a disease-causing mutation without symptoms have "latent" porphyria. However, this does not mean that such an individual will never have symptoms. Genetic factors (that is, the presence of a porphyria-causing gene mutation is not the only factor involved. Exposure to certain environmental factors, such as drugs, chemicals, diet, and sun exposure can, depending on the type of porphyria, greatly influence whether an individual with a mutation in a porphyria-causing gene has symptoms and the severity of symptoms. There may also be additional factors, including additional genes, that may modify the symptoms. This is why it is important that all family members of individuals diagnosed with porphyria be tested whether they have symptoms or not, and that all individuals who have a confirmed diagnosis of porphyria be educated about and follow the recommended precautionary and preventive measures for porphyria.
Where can I find a porphyria expert? What other type of doctor can diagnose me properly and what type of specialist should I see if I have porphyria. There are several Porphyria experts in the US and outside the US, including the Porphyria Centers in this Consortium. Information about other experts can be obtained by contacting the American Porphyria Foundation (www.porphyriafoundation.com) or one of the Porphyrias Consortium members. If a porphyria is suspected, any physician can order the appropriate tests. Since interpretation of these results may be difficult, it is best for the physician or healthcare professional to consult with a porphyria expert for an accurate interpretation of the results and, if necessary, advice about additional testing, treatment, or prevention and precautionary measures.
Can I have more than one type of porphyria? Because all porphyrias are uncommon, it is very unlikely that more than one type of porphyria will occur in the same family, or that a person with one type of porphyria will go on to develop another type. However, patients with more than one type of porphyria have been reported.
Can porphyria improve with age? The symptoms of porphyria do not improve with age, per se. Untreated, the symptoms and the secondary effects of long-term symptoms will get worsen over time. However, with proper diagnosis, treatment of acute attacks (in the acute porphyrias), and following recommended preventive measures, it is possible that symptoms may be lessened.
Should I be tested often? How often? Monitoring of porphyrin levels and other follow-up testing is dependent on the type of porphyria and the medical status of the individual. It is, therefore, important that a person who has been diagnosed with porphyria be followed by a porphyria expert.
Does porphyria affect my liver? Should I have liver tests? Liver function tests should be performed routinely on all individuals diagnosed with porphyria.
Do people have liver transplants for poprhyria? Liver transplantation may be beneficial for individuals with end-stage liver disease as a result of porphyria.
My doctor diagnosed me with porphyria but the porphyria expert said I did not have it. Why would this happen and should I be retested? Such a situation needs to be dealt with on an individual basis. Whether further testing is recommended depends on how the patient was initially diagnosed and how the porphyria expert made the decision that porphyria is not the diagnosis. The results of biochemical testing are sometimes interpreted incorrectly by a physician who is not an expert in porphyria. Review of the results of the biochemical testing by a porphyria expert may determine that the results are not consistent with what is typically seen in a patient with porphyria during an attack. The results of DNA analysis may also contribute to the porphyria expert saying that it is unlikely that the patient has porphyria. DNA analysis, although considered to be the gold standard for diagnosis, is not perfect in that the patient may have a mutation in a part of the porphyria gene that is not analyzed by routine testing or the patient has a mutation in a porphyria gene that was not analyzed. In the event that a diagnosis of porphyria is still suspect, then it is recommended that the patient undergo additional biochemical testing at the time of an acute attack. Additionally, further testing may include DNA analysis for other acute porphyrias (if only one or two were tested).
Is porphyria research being conducted? How can I volunteer to participate in research?
Yes. For additional information about research being conducted and how to volunteer to participate, please contact either the Porphyrias Consortium Coordinator by email (porphyria.center@mssm.edu) or telephone (212-659-6779) or one of the site coordinators (see list of Porphyrias Consortium Members for locations and contact information).
Acute Porphyrias
Does surgery or pregnancy pose additional risks? Porphyria-related risks of surgery and pregnancy depends on the type of porphyria. Surgery may increase the risk of an attack of the acute porphyrias. This risk can be greatly reduced if certain precautions are taken, including the type of anesthesia used. The patients surgeon and anesthesiologist should consult a porphyria expert prior to hospitalization for surgery. Such consultation may also be helpful during pregnancy. Although attacks of acute porphyria can occur during pregnancy, the risk appears to be less than formally thought. Treatment of acute attacks during pregnancy is feasible.
What drugs are safe and unsafe? For information about safe and unsafe drugs in the acute porphyrias, it is best to consult the American Porphyria Foundation Acute Porphyrias Drug Safety Database (http://www.porphyriafoundation.com/drug-database) or the European Porphyria Initiative (http://www.porphyria-europe.org/03-drugs). The databases contain expert assessments of the potential of drugs to provoke attacks of acute porphyria (AIP, VP, HCP & ADP) based on the available evidence. However this evidence is not always complete, which may lead to some degree of uncertainty. The information in these databases is meant as guidance to health care professionals. It must be made clear that the prescription of drugs to a patient with acute porphyria is entirely at the risk of the physician in charge.
Since most commonly used drugs have not been tested, they should be avoided if at all possible. If a question regarding drug safety arises, a physician or medical center specializing in porphyria should be contacted.
Can men have acute porphyria? Yes. Since the acute porphyrias are inherited in an autosomal dominant pattern, males and females are equally at risk for having an acute porphyria. Exposure to certain environmental factors, such as drugs, chemicals, and diet, greatly influence whether an individualmales and females--with a mutation in a porphyria-causing gene has symptoms and the severity of symptoms. However, one of the environmental is hormones, and, therefore, attacks are more common in women than in men. Women may experience cyclical acute attacks associated with their menstrual cycle, starting in puberty. Such attacks in women may occur after ovulation and during the last part of the menstrual cycle when progesterone levels are high.
Do I need a special diet with porphyria? Nutritional recommendations for the acute porphyrias emphasize a high carbohydrate intake as part of a balanced diet that provides all essential nutrients. The recommendations include an adequate intake of dietary fiber, vitamins and minerals. The goals are to prevent acute attacks of Porphyria that may be related to diet, avoid deficiencies of nutrients, and maintain a normal body weight. More information on diet on theAmerican Porphyria website (http://www.porphyriafoundation.com)
Will porphyria affect my thinking and memory? Generally, the acute porphyrias do not affect thinking and memory. However, a person may experience some neurological effects, including confusion, convulsions, muscle weakness, and, rarely, paralysis, due to effects on the nervous system.
What precipitates a porphyria attack? In an individual with an acute porphyria, an acute attack can be brought on by certain drugs, hormones in women, environmental factors including chemicals of various types, nutrition including fasting and low carbohydrate diets, alcoholic beverages, medical and physical stress, and physical fatigue.
I have acute porphyria: Can I do the following: take a flu shot, donate my organs, take aCAT scan with the contrast? Flu shots are not contraindicated for individuals diagnosed with acute porphyria, and can be taken safely. Any immunizations appear to be okay. In fact, since other illnesses can bring on a porphyria attack, remaining healthy is one of the most important ways to prevent acute attacks.
There has been no information to date to suggest that CAT scans with or without contrast agents should not be performed on an individual with porphyria.
Organ donation would be up to a particular transplant program or network. In acute porphyrias any organ should be acceptable except perhaps the liver. In the case of PCT organ donation would most likely be acceptable in the absence of a history of hepatitis C or HIV.
What should I do if the drug I need is on the unsafe list? Drugs on the unsafe list are those drugs that should be avoided by individuals diagnosed with an acute porphyria because they have been found to provoke an acute attack in some individuals. If a drug prescribed for an individual diagnosed with an acute porphyria is on the unsafe list, the prescribing physician should check the Drug Database for a safe alternative. No drug should be withheld if it is judged essential for optimum treatment of a life-threatening condition (e.g. chemotherapy for cancer). The risk versus the benefit should be assessed and discussed with the patient. For help with this assessment you may wish to contact a Porphyria expert. It may be recommended that a patient undergo biochemical monitoring in the early stages of treatment It must also be noted that response to drugs in patients with an acute porphyria is extremely variable and individuals may be encountered who have used an unsafe drug without adverse effect.
Cutaneous Porphyrias
Is sunlight always harmful? Sun sensitivity can occur in all but two types of porphyria, specifically AIP and ADP. The degree of sensitivity to sunlight varies considerably. Patients with sun sensitivity have high levels of porphyrins in the blood plasma which, depending on the type of porphyria, have originated from the liver or the bone marrow. Ultraviolet light interacts with porphyrins in such a way as to damage skin tissue. Some treatments may help patients tolerate sun exposure even without lowering porphyrin levels. In some cases, treatment can lower porphyrin levels and sunlight can be tolerated.
Should I use a special sunscreen? Most patients with a cutaneous type of porphyria must learn to avoid sunlight as much as possible. Protective clothing may also be recommended. For patients with EPP, treatment with pharmaceutical grade β-carotene (Lumitene, Tishcon) or cysteine may improve sunlight tolerance but does not lower porphyrin levels. Over-the-counter sunscreens and over-the-counter beta carotene (vitamin A) is not effective.
·Causes of Insomnia:Do you know what's keeping you up at night? Learn why people can't sleep.
Tips to Fit Your Sleep Style
Did you know your sleep style takes on a personality? Even if you are sleep-deprived, what you do in the hours before bedtime, whether you smoke or drink alcohol, even how much you weigh, can all affect how much and how well you sleep.
If your sleep isn't great right now, see if any of these "sleep styles" noted by the National Sleep Foundation sound like you.
Dragging Duos
Most poor sleepers fit into this category. You get up early, put in long hours on the job, and bring your work home, sometimes working almost up until bedtime. You know you don't get enough sleep, and neither does your partner. You try to make up for lost sleep on the weekend.
These tips may help:
·Power down before bedtime.It can be hard to resist the temptation to check your email one last time. "Computer screens emit a bright light that signals the brain to wake itself up," says Michael Decker, PhD, ABSM, who is the spokesman for the American Academy of Sleep Medicine. So stop any computer work, emails, and other screen activities at least an hour before bed.
·Create a wind-down ritual.While you're awake, you may want to get things done. But relaxing can help set the stage for sleep. At least an hour before bedtime, read, listen to music, play with your pet, stretch, or do something else that relaxes you.
·Limit naps."Naps and sleeping a little longer can help you catch up on the weekend, but that still leaves you sleepy throughout the week," says Russell Rosenberg, PhD. He is chairman of the National Sleep Foundation.
·Make sleep a priority.It's that simple, and that essential. Every night counts.
Overworked, Overweight, and Overcaffeinated
"These are people trying to cope with very high demands in their life," Rosenberg says. They tend to work the longest hours (often on night shifts or rotating shifts) and get the least sleep.
If this sounds like you, you probably think you function well on little sleep, though you likely also lean on caffeine. You're also more likely to smoke, drink alcohol, and be obese, and may well have trouble sleeping.
These tips may help:
·Limit caffeine to the morning.Its effects can last for hours after you drink it.
·Stop smoking.Nicotine is a stimulant, notes Decker. It promotes inflammation in the back of the throat, which can lead to snoring or sleep apnea. Sleep apnea -- lapses in breathing during sleep -- is harmful itself and can lead to insomnia and other health problems.
·Lose extra weight.Here's another reason to shed extra pounds:Lack of sleep and obesity can go together. Being sleep deprived can affect your metabolism, and obesity can give you sleep apnea, a cause of insomnia. Working on your weight can pay off with your sleep, Rosenberg says.
·Get help for chronic insomnia.If you have difficulty falling or staying asleep 3 nights a week or more, and that persists even after you change your sleep habits, see your doctor.
Missing Sleep and Your Partner
You drag during the day and are sometimes too sleepy for intimacy.
You may sleep separately from your partner and you may worry. You may be depressed or anxious, too. You have a hard time falling asleep and sometimes use sleep medications.
These tips may help:
·Don't rely on over-the-counter sleep medications. Treating sleep problems usually involves lifestyle changes, building better sleep habits, and treating any conditions that are affecting your sleep.
·If you're depressed, get help. Sleep and depression have a complex link. Depression can cause sleep problems and vice versa. Insomnia is especially common with depression, and treatment can ease both.
·Share your bedroom. Most partners want to sleep in the same room. Start working on the issues that keep you apart.
Healthy, Lively Larks and Sleep-Savvy Seniors
These two types of sleepers are least likely to have sleep problems and most likely to get enough or more than enough -- sleep. They rarely or never feel tired. If you're a lively lark, you're probably a young, early riser and don't have any medical conditions. If you're a savvy senior, you may be retired, get up later than average, and supplement nighttime sleep with naps.
This tip may help:
·Don't take sleep for granted. Keep up good sleep habits, especially as you age. "When you're younger, you may be able to have two pots of coffee in the afternoon and sleep fine, but abuse of stimulants can catch up with you and cause problems later," Rosenberg says.
Remember Research is the key to your cure!
Inside Clinuvel: Porphyrins & Porphyrias 2013
Wednesday - May 29, 2013 @ 22:55:55
Inside Clinuvel: Porphyrins & Porphyrias 2013
The biennial Porphyrins & Porphyrias conference is the only international meeting of global key opinion leaders on the group of diseases known as porphyrias. Convening last week (15-19 May) in Lucerne, Switzerland, P&P has become an important fixture on Clinuvels calendar, providing an opportunity to review updates from across the globe and discuss our program with international experts.
Our specific interest in the porphyrias lies with erythropoietic protoporphyria (EPP), one of the rarer forms of the disease grouping and the lead indication for our drug SCENESSE (afamelanotide 16mg implant). Indeed there were a number of presentations reviewing updates in thinking on EPP, including presentation of results from Clinuvels program. Ill return to those shortly, however, as there have been significant advances in another form of porphyria and it would be remiss not to at least mention these here.
Porphyrins and pathways
Porphyrias are diseases which arise due to genetic defects. If the specific genetic material is passed from both parents, a child will be born with a porphyria. In some instances, porphyrias can also be acquired due to chemical exposure or secondary diseases leading to similar genetic malfunctions. What is common to all porphyrias, however, is the accumulation of molecules in the body known as porphyrins or porphyrin precursors due to a malfunction in the pathway by which the body produces haem (heme). The accumulation of these molecules can then lead to acute and chronic symptoms in porphyrias, often onset by a trigger.
In EPP, for example, the phototoxic molecule protoporphyrin IX (PPIX) is accumulated in the skin which, when triggered by exposure to visible light, causes unbearable, untreatable attacks of dermal pain which can last for several days.
Advances in genetic therapy for acute porphyrias
In acute porphyria, the accumulation of other porphyrins and/or their precursors can lead to acute attacks on other organs, often presenting as nausea, vomiting and severe abdominal pain for which narcotics are often the recommended therapy. While a therapy exists a haem arginate product is often used in these patients as a preventative and responsive therapy acute porphyrias have long been considered as viable candidates for gene therapies which would better help manage their disease and eliminate or reduce the need for other therapies. At the 2011 P&P conference in Cardiff the gene therapies were discussed in depth, however this year preliminary observations from two teams were reported for the first time. The first is already in human clinical trials with a small cohort of patients being treated across Europe, while the second reported successful results in animal models with the plan to commence human studies in the coming year. Both teams reported encouraging data and/or anecdotes from their work. While many steps will need to be taken before conclusive evidence of the safety and efficacy of genetic therapy is at hand, it is indeed exciting to view these important advances for rare disease patients.
On EPP
In addition to the buildup of the phototoxic molecule PPIX in the skin in EPP, PPIX can also accumulate in the liver, leading to liver failure in a small number of patients (you can view one EPP patient discussing her experiences with liver transplantation following liver failure on our YouTube channel here). Traditionally quoted as 1-4% or about 5% of patients, the reality is that the chances of liver failure in EPP are not really understood, nor is it possible to predict which patients may suffer from liver failure. Presenting this in some depth, Dr Staffan Wahlin from the Karolinska Institute highlighted that there is still much to learn about liver toxicity in EPP and that patients needed to be closely monitored, perhaps every 6-12 months, as well as counseled on the traditional risk factors for liver failure.
Data from Clinuvels European Phase III confirmatory study (CUV029) of SCENESSE in EPP were presented in an oral abstract by Dr. Janneke Langendonk of the Erasmus MC University Hospital, Rotterdam, representing the eight study centers which took part. After closely reviewing the studys setup and objectives, Dr Langendonk gave a review of both the statistical results and the reports from her patients, acknowledging both indicated a positive efficacy profile for the drug. Dr Langendonk also reviewed the safety profile of afamelanotide in EPP from her experiences, suggesting that the adverse events seen in the studies which were drug related were not serious.
A collaborative response
For the second time in the P&P conferences history, the final day of presentations was devoted to an international porphyria patient day encouraging interaction between both physicians and patients to gain a better understanding of the porphyrias. In all, more than a dozen nations were represented in the room, with presentations on all forms of porphyrias simultaneously translated from English to German.
For me, this international delegation gave the best indication yet that the community surrounding porphyria research clinicians, patients and industry has dramatically improved its ability to collaborate across borders with the goal of finding therapies for porphyria patients. Initiatives such as EPNET, the American Porphyrias Consortium and the Protect Our Future program have gained traction in recent years and are better integrating to achieve common goals. This kind of approach is vital in rare diseases which are difficult to diagnose, lack effective treatments and are generally poorly understood by those outside the immediate field. Well be working hard to assess the role of Clinuvels drug as an effective therapy for patients who need it most.
- Lachlan Remember Research is the key to your cure!
How To Have A Bad Day Gracefully And Avoid Guilt With Chronic Illness
You wake up and flip over (if you even slept that night) and you know by just that slightest movement that it is going to be a long, draining, and painful day. At that point you have to make several decisions. Do I get out of bed or do I stay in bed longer and get some rest? Should I stay in my pajamas or do I use what little energy I have right now and get dressed for the day? Do I got to work or do I call in and use one of my sick days? As someone that has a chronic illness you have to make more choices then the average person. I have always envied those that could just pop out of bed and do their morning routine thoughtlessly and on autopilot. Envy is not a good emotion nor is a bad attitude first thing in the morning so I had to make some changes to how I managed my mornings and I thought I would share them with you.
GRATITUDE
When you arise in the morning, think of what a precious privilege it is to be alive to breathe, to think, to enjoy, to love. ~Marcus Aurelius~
Mornings set the tone for your entire day so it is good to be mindful of your thoughts and words in the morning. Giving thanks that you are alive and that you have been blessed with a new day on this earth is a great way to start the morning. I simply say Thank you when I awake. You can thank your God, The Universe, or even spouse or family member for just being in your world. There is a connection between gratitude and health that goes back a long way.
Grateful people tend to be more optimistic, a characteristic that researchers say boosts the immune system. There are some very interesting studies linking optimism to better immune function, says Lisa Aspinwall, PhD, a psychology professor at the University of Utah. In one, researchers comparing the immune systems of healthy, first-year law students under stress found that, by midterm, students characterized as optimistic (based on survey responses) maintained higher numbers of blood cells that protect the immune system, compared with their more pessimistic classmates.
Optimism also has a positive health impact on people with compromised health. In separate studies, patients confronting AIDS, as well as those preparing to undergo surgery, had better health outcomes when they maintained attitudes of optimism.
People are like stained-glass windows. They sparkle and shine when the sun is out, but when the darkness sets in their true beauty is revealed only if there is light from within.
~Elisabeth Kübler-Ross~
If you are in a flare (a increase of pain or symptoms) make sure to set realistic goals for the day. Not completing what you intended to do can bring on a flood of negative emotions that will just make you feel worse. Remember not to attach your self worth to what you can and can not finish that day. It is great to have goals even during a flare but you need to be realistic about what you can accomplish. Yesterday you might have been able to walk a mile and today you might only be able to go to your mail box and that is okay because you did something! Staying in bed I think is the worst thing you can do. It gives you to much time to think about the pain. Even if you go from the bed to the sofa to watch a movie to cheer you up it is better then staying in bed all day. By doing things that you enjoy you can distract yourself from your symptoms. Try to keep your mind busy and take a couple naps! You will find you are not as focused on the illness if you keep your mind occupied.
DONT FEEL GUILTY IF YOU HAVE TO CANCEL PLANS
A true friend is one who thinks you are a good egg even if you are half-cracked.
~Author Unknown~
One thing you do find out having a chronic illness is who your real family and friends are. Breaking plans is always a unpleasant experience that no one likes to do but if you can barely walk, that trip to the zoo is most likely not going to happen. It can be very disappointing for both parties involved. Feeling guilty or someone else making you feel guilty about something that is out of your control can really take a blow at your self esteem. People sometimes say some not so nice things when you break plans with them. Their feelings are THEIR FEELINGS and they are entitled to them. How you react to it or let it effect you is your choice. No one can make you feel guilty about it but you. It is not a easy thing to do but it is possible. When you start to get those feelings of guilt tell yourself you did nothing wrong and you are doing the best thing for your body right now. It is important to remind yourself that it is okay you broke plans because it was the best thing for you to do so that you can start your path to healing your body.
BE KIND TO YOURSELF AND TO OTHERS
Treat everyone with politeness, even those who are rude to you not because they are nice, but because you are. ~Author Unknown~
When you are having a bad day you need to be extra kind to yourself . Although this might sound selfish it is necessary to take extra good care of yourself when you are in a flare. Be kind to your body and eat healthy foods. Be kind to you mind and soul by doing things that you enjoy. Reading a book, crocheting, listening to music, or taking a short walk outside whatever makes you feel better on the inside. If you feel better on the inside you will physically start to feel better. It is also important to continue to be kind to others. I wrote a blog post a few weeks ago about this very subject Do I have the right to be unkind because I am sick? kindness actively changes your bodys biochemistry to produce positive chemicals, you can change both your psychological and physical responses through giving/receiving kindness. Positive emotional experiences help soothe your body, reduce stress and improve your sense of well-being and it also makes you and the other person feel good.
Dont rely on someone else for your happiness and self worth. Only you can be responsible for that. If you cant love and respect yourself no one else will be able to make that happen. Accept who you are completely; the good and the bad and make changes as YOU see fit not because you think someone else wants you to be different.
~Stacey Charter~
Remember Research is the key to your cure!
New Panhematin brochure available for your physicians.
Tuesday - May 28, 2013 @ 17:03:09
New Panhematin brochure available for your physicians.
Panhematin
The APF has produced a new Panhematin brochure. If you would like a copy of the new brochure for your physician, please contact the APF and we will forward one to you promptly. Remember, too, that the APF will send your doctor a complimentary comprehensive doctor packet for the acute porphyrias. Call 1.866.APF.3635 or email porphyrus@aol.com . If your physicians have questions about the administration or use of Panhematin, we will then send an instruction form or arrange a consultation with a porphyria expert if needed.
For the many patients who are taking Panhematin, please note that Recordati Rare Diseases, Inc. has purchased Panhematin from Lundbeck Pharmaceutical. Recordati Rare Diseases, Inc. has assured us that there should be no interruption in receiving the Panhematin treatment and that the product is the same as it has always been. In fact, for the next number of months, the telephone numbers and delivery services that were available through Lundbeck Pharmaceutical will remain the same, as well.
FYI For questions from healthcare professionals regarding general use and administration of Panhematin, please call Recordati Rare Diseases at 1-866-402-8520. Your call will be answered by a member of the Lundbeck staff on behalf of Recordati Rare Diseases until late 2013. Your physician or hospital pharmacy can order Panhematin through a wholesaler of their choice. Healthcare professionals can call 1-888-514-5204 to receive help with regular and emergency shipments, Monday thru Friday, 9 am to 6 pm EST. After hours and emergency orders, call1-800-673-6723. In an emergency event, when the hospital/physician/wholesaler does not have Panhematin in stock, Recordati Rare Disease will ship directly from its Lavernge, TN distribution site via an expedited delivery service to anywhere in the U.S.-usually within 12-14 hours.
During the 2013 International Porphyria Congress Patient Day meeting, Dr. Jean Charles Deybach spoke about the great benefit of early treatment withheme therapy ( Panhematin and Normosang)
Rapid clinical improvement.
Decreased urinary ALA/PBG 2-3 days
Mean abdominal pain duration 2-3 days
No further severe neurological complications
No major side effects in acute administration
Safe use during pregnancy (Badminton & Deybach, 2006; Marsden & Rees, 2010)
Remember Research is the key to your cure!
Rare Diseases Info & Advocacy Did you know!
Tuesday - May 28, 2013 @ 17:00:11
Rare Diseases Info & Advocacy
A rare disease in the United States is one that affects fewer than 200,000 people. As anyone who has searched for a diagnosis or suffered from a rare disease knows, it's easy for these illnesses to get lost in the crowd of more common conditions like cancer, heart disease and diabetes. There is little incentive for healthcare professionals to learn the details of treating a disease when they may see only one or a handful of patients with it throughout their careers. From the drug makers' perspective developing products for a small and unfamiliar market is not terribly attractive. And with so many diseases that affect millions vying for scientific and clinical research money from government and other funders, small diseases like Porphyria can be easily forgotten. Nearly 30 years ago, the APF took action to make sure that Porphyria, and rare diseases generally, would receive attention in Washington. The APF joined people like Marjorie Guthrie (widow of the great American folk-singer Woody Guthrie, who died in his 40s of Huntington's Disease) and other rare disease advocates to form the National Organization for Rare Disorders (NORD). Actor Jack Klugman helped give the campaign for rare diseases awareness national prominence, featuring the rare disease problem on two episodes of his program Quincy, M.E., and testifying before Congress. In 1983, President Reagan signed the Orphan Drug Act into law, and the FDA established an Office of Orphan Products Development. The NIH Office of Rare Diseases was established in 1993, so two agencies now share responsibility for ensuring that rare disease research and treatment needs remain on the Federal health care agenda. Remember.Research is the key to your cure!
A Story From James Beadles with EPP
Tuesday - May 28, 2013 @ 16:55:55
James Beadles
Type of Porphyria:
Erythropoietic Protoporphyria (EPP)
I live life with EPP! I was diagnosed when I was six by a dermatologist named Carl Anderson who has since passed away. Up until my diagnosis, my parents had heard it all from a number of doctors. I was allergic to a medicine, or I was allergic to weed killer, to simply saying, "it is just a rash." All the while, I would scream in pain. My parents would help by placing cool clothes on me. I live in sunny southern California in a beach town. All my friends were into surfing and sailing. The outdoors is part of life in SoCal. I did not let my EPP stop me from enjoying the outdoors though sometimes I paid dearly. I played baseball until high school. I learned to sail. I ran in triathlons and half-marathons. I snow skied and water-skied. I played golf. All the time I endured the funny looks and mean things said about the way I looked and had to dress. I did not let it stop me. Sure, it bothered me when I was young. It hurt. However, as I got older I saw it as other people's problem, not mine. I was living my life the best way I knew how. I was not going to let EPP stop me from enjoying life. I had a doctor once who told my parents I should move to Seattle where it was cloudy more often. He said I should learn to play chess and ping-pongindoor sports instead of baseball and golf and sailing. My parents would hear nothing of it; they knew I was going to live my life the way I wanted to live. I have had two liver transplants because of my EPP. The porphyrins dumped into the liver and made it cirrhotic. I had my first transplant when I was 27 years old. The liver lasted 12 years, during which I was able to continue my normal active lifestyle. I married and had two kids. Neither of my kids shows symptoms of EPP. In fact, one wants to be a lifeguard! Both of my children can run around on the beach all day without being burned, well, aside from basic sunburn. Their mother and I lather them with sunscreen when they go out to the beach or are playing soccer or swimming. The boys are six and eight and I am confident they do not have EPP. My second transplant was more dramatic. I was 39, my liver and kidneys failed, and I went into a coma. I was transplanted three weeks later and subsequently spent the next eight months in UCLA Medical Center. I was on dialysis for six months after which by some miracle my kidneys began to work again. The transplant and hospitalization took a great toll on my body. I am no longer able to be as active as I was. I have neuropathy in my feet from the kidney failure and nerve damage from being in bed for so long. I am twenty pounds underweight and weak. I like to joke that I am a 42-year old living in a 92-year-old body. I still live with the EPP and who knows how long this liver will last. I take infusions of Panhematin to slow the progression of porphyrins into the liver (this is the hope anyway). The key is I am still living. I still endure the looks from people, like the other parents at the soccer field when I watch my kids play. I do not care if they think it is odd someone wearing long pants, long sleeves and gloves on a 90-degree SoCal day. To me, they have a problem, not me. People do what they have to do to cope. I am not going to let EPP keep me from enjoying my life and enjoying watching my kids grow up. My kids understand that Dad has to be careful of the sun. They understand Dad is not as strong as he once was because of his surgery. They understand why Dad has to wear protective clothing in the pool; they are just happy that Dad is in the pool with them! Grown-ups should be so understanding. I hope you enjoy my story and I am anxious to hear how others with EPP are LIVING, not just coping or suffering. Someday there will be a cure for this, and I plan on being around to see it!
Remember.Research is the key to your cure!
Take Good Care of Your Body - It's the Only Place You Have to Live
Sunday - May 26, 2013 @ 18:11:33
Take Good Care of Your Body - It's the Only Place You Have to Live
Many people go through life not taking any responsibility for their own health. They drift along until something goes wrong then it is off to the doctor to get it fixed. It seems that people take better care of their car than their body and get it serviced regularly so it doesn't break down.
You should think of your doctor as really just the breakdown service when the wheels fall off. What you do on a day to day basis is your 'self care' or maintenance and each of us is responsible for our own. Without this maintenance real health can never be achieved and real health is a great deal more than just 'not being sick' or an absence of disease.
Real health is about peak performance physically, mentally and emotionally. You have a high level of strength and energy, emotional balance, a lean slim body, and a sharp and nimble mind. Your strong healthy body has the ability to fight off disease and illness that stalks and pounces on so many people cutting their lives short after years (even decades) of pain, disability and ill health.
Diseases such as heart disease, cancer and diabetes are labeled 'lifestyle' diseases, caused by the way you live your life. Caused by what you do and don't do each and every day in the way of proper nutrition and proper exercise. These diseases are preventable and rob families of their loved ones well before their time.
It is important that our life span is also matched by our health span. Our health is important and we tend to take it for granted until we find ourselves out of health. The knowledge about what it takes to remain healthy and well is vastly increasing every year, which has enabled people to live longer, and to treat more illnesses.
Yet we are producing children today that are now unhealthier and may even die before their parents. It is a sad fact that children being born today are predicted to have a 20-30 year shortened lifespan.
Deficiencies create situations in which millions of people world wide function well below their potential. These deficiencies are lack of proper nutrition and proper exercise. It can mean your blood doesn't pump efficiently, your digestion doesn't break down food properly, your weight keeps increasing, you have constant aches and pains, don't feel well, aren't sleeping properly, are depressed and the list goes on.
Yet your health cannot be left for your doctor to take care of. Your doctor does not look after your health; your doctor only looks after your illnesses. If your doctor says you are well and healthy it means that things have not got so bad that there are enough actual symptoms for a disease diagnosis.
But this can also mean a person it still far from being 'well' and they usually do not feel well either. In fact they are often called the 'walking wounded' as they are not sick enough to be bedridden (yet) but not well to function properly either.
It has been estimated 80 percent of diseases are caused by the lifestyle choices we make every day. Many people have good intentions and mean to get started on a proper exercise program and eat better but the trouble is it is much easier to put off doing things until tomorrow, and for many tomorrow never comes.
So what are you doing, now, today? Are you working on keeping your muscles and bones strong with strength training exercise a couple of times each week? If not give yourself a good talking to and get yourself started so your body doesn't let you down somewhere down the track. It is all about prevention not waiting till there is a problem then looking around for someone to try and fix it as it will likely be way too late.
Remember - take good care of your body - it is the only place you have to live.
Remember.Research is the key to your cure!
Dont worry, be happy: Tips to relieve anxiety
Wednesday - May 22, 2013 @ 23:43:35
Dont worry, be happy: Tips to relieve anxiety
Anxiety can often be crippling. The next time you are anxious, find relief with these techniques.
Drive away you anxieties!
Anxiety and worry can lend a helping hand if it can spur you to action. But if youre constantly anxious it can be a difficult problem as it will become a hindrance to everyday life rather than motivate you to do better. It can sap you off all your energy, leaving you feeling powerless.
Self-help techniques for anxiety relief:
The next time you find yourself in that place, heres what you can do to jump out of there.
Breathe: Thats the best thing you can do to slow down. Take a few minutes, close your eyes and breathe deeply. Inhale slowly through your nose, hold your breath for a few seconds and breathe out slowly through your mouth. Do this at least 4-5 times and youll instantly feel relaxed.
Put your thoughts down: When youre anxious or worried, your mind is clogged with numerous what ifs and worst-case scenarios. Putting them down brings about clarity and also provides a safe place to vent out.
Dont worry, be happy: Tips to relieve anxiety
Anxiety can often be crippling. The next time you are anxious, find relief with these techniques.
Drive away you anxieties!
Anxiety and worry can lend a helping hand if it can spur you to action. But if youre constantly anxious it can be a difficult problem as it will become a hindrance to everyday life rather than motivate you to do better. It can sap you off all your energy, leaving you feeling powerless.
Self-help techniques for anxiety relief:
The next time you find yourself in that place, heres what you can do to jump out of there.
Breathe: Thats the best thing you can do to slow down. Take a few minutes, close your eyes and breathe deeply. Inhale slowly through your nose, hold your breath for a few seconds and breathe out slowly through your mouth. Do this at least 4-5 times and youll instantly feel relaxed.
Put your thoughts down: When youre anxious or worried, your mind is clogged with numerous what ifs and worst-case scenarios. Putting them down brings about clarity and also provides a safe place to vent out.
Take a hot bath: A hot bath can be very soothing. Add some bath salt and just soak in. If you can, light some aromatic candles, play some ambient music and create your own safe get-away place in your bathroom. If you dont have a bath tub, you can still light some candles, play music and take a hot shower. Visualise the water washing away all you worries and anxieties, this exercise is known to be very effective.
Stay away from caffeine: Tough one, isnt it? Caffeine being a stimulant can further propel anxiety and worries. So steer away from coffee and black tea and do yourself a favour.
Sip on herbal teas: Alternatively, try some soothing teas. Rose tea, green tea, chamomile or other such herbal teas can be very helpful when youre worried. They can help calm you down and soothe your worries.
Bite into a chocolate: Chocolate releases feel-good chemicals that make you happy, one of them called phenylethylamine, is released when you fall in love. So they next time you feel youre down in the dumps with worries and anxiety, bite into a piece of yummy chocolate for some instant relief. Dont make it a habit though and make sure you address the cause of that anxiety once youre calm.
Try visualisation: This technique is hailed as an effective means of stress relief. So when youre feeling anxious, close your eyes and try a guided imagery. First breathe deeply and relax.
Heres one visualisation you could try:
§Picture a serene setting such as a clear blue sky, grass fields, an angular tree, and a soft stream.
§Imagine yourself sitting there.
§Go over all the things that are worrying you.
§Feel the height of emotions youre experiencing.
§Imagine throwing away each worry into the stream. See it dissolve in the water.
§Once youre done discarding each of those worries you have, imagine walking over to the stream.
§Take a dip in that stream of fresh, cool water� Watch any residual worry wash away.
§Walk back, and visualise the glowing sun dry you.
§Come back to reality and rest for a bit before you jump into anything else.
Go for a walk: A ten-minute walk can be very relaxing. Concentrate on your breathing while youre at it. And try and stay mindful.
Aroma therapy: Certain fragrances can be emotionally uplifting. Light an incense stick, or a scented candle. If not that, you can also put a few drops of your favourite scent onto as napkin and take a whiff. Choose between lavender, jasmine and rose, as they are known to be relaxants. Now go, calm yourself with a soothing fragrance.
Take a hot bath: A hot bath can be very soothing. Add some bath salt and just soak in. If you can, light some aromatic candles, play some ambient music and create your own safe get-away place in your bathroom. If you dont have a bath tub, you can still light some candles, play music and take a hot shower. Visualise the water washing away all you worries and anxieties, this exercise is known to be very effective.
Stay away from caffeine: Tough one, isnt it? Caffeine being a stimulant can further propel anxiety and worries. So steer away from coffee and black tea and do yourself a favour.
Sip on herbal teas: Alternatively, try some soothing teas. Rose tea, green tea, chamomile or other such herbal teas can be very helpful when youre worried. They can help calm you down and soothe your worries.
Bite into a chocolate: Chocolate releases feel-good chemicals that make you happy, one of them called phenylethylamine, is released when you fall in love. So they next time you feel youre down in the dumps with worries and anxiety, bite into a piece of yummy chocolate for some instant relief. Dont make it a habit though and make sure you address the cause of that anxiety once youre calm.
Try visualisation: This technique is hailed as an effective means of stress relief. So when youre feeling anxious, close your eyes and try a guided imagery. First breathe deeply and relax.
Heres one visualisation you could try:
§Picture a serene setting such as a clear blue sky, grass fields, an angular tree, and a soft stream.
§Imagine yourself sitting there.
§Go over all the things that are worrying you.
§Feel the height of emotions youre experiencing.
§Imagine throwing away each worry into the stream. See it dissolve in the water.
§Once youre done discarding each of those worries you have, imagine walking over to the stream.
§Take a dip in that stream of fresh, cool water� Watch any residual worry wash away.
§Walk back, and visualise the glowing sun dry you.
§Come back to reality and rest for a bit before you jump into anything else.
Go for a walk: A ten-minute walk can be very relaxing. Concentrate on your breathing while youre at it. And try and stay mindful.
Aroma therapy: Certain fragrances can be emotionally uplifting. Light an incense stick, or a scented candle. If not that, you can also put a few drops of your favourite scent onto as napkin and take a whiff. Choose between lavender, jasmine and rose, as they are known to be relaxants. Now go, calm yourself with a soothing fragrance.
Remember.Research is the key to your cure!
How Karen Eubanks was encouraged with the In-Touch Program
Wednesday - May 22, 2013 @ 23:40:40
Karen Eubanks
Type of Porphyria:
Acute Intermittent Porphyria (AIP)
My Hero, by Haley Eubanks photo: Mother & Daughter, Karen and Haley Eubanks Growing up, I've always had the fear of losing my mom. She's the strongest person I know and what makes her so strong is the will power and strength God gave her. My mom has a rare disease called acute intermittent porphyria. There's no cure, but there is a medicine called Panhematin that my mom receives every week through a port. This medicine controls her attacks, which she has every 21 days. There has been two times where I thought she was gone and the day would come that I dread the most. When I was in kindergarten, my mom quit her job. I remember her telling me she was sick and wasn't able to work anymore. Since I was five years old, I didn't quite understand, and as time progressed the sickness never left. I knew then that the sickness would never leave. I remember coming home and my mom not being there. I was attached to my mom, like any other young child and her not being there felt like something was always missing and a part of me was lost. No one would explain to me what was really going on because of my age. I remember seeing her in the hospital and thinking that wasn't my mom. But it was, just a different view of her-a view a child never wants to see of their mom. I only went to the hospital twice because my family wanted to keep me focused and not startle me. My grandmother, my mom's mom, was like a second mother to me. It was hard being around her at times because she reminded me exactly of my own mom. Looking at my grandmother, during that time, was hard because her face was discolored, worried, and full of pain. I stayed with my grandmother during the whole time that my mom was in the hospital, because our family was at loose ends with what the disease was putting us through. As time progressed, my mom returned home. I'm not sure how long she stayed at the hospital but it was for over three months and as a child I told people it felt like forever. When she came home, she stayed for quite some time before going back into that negative stage. In my sophomore year, I was going through drama with friends and I wasn't on top of my game in soccer. By this time I fully understood my mom's disease even though I had to bug people, I still received answers. During February, my mom was thrown into an attack that left her in ICU. When going to see my mom in ICU, she didn't know who I was, she couldn't talk, and her skin made her appear as if she was already dead. The condition she was in was unbearable for me and thinking about the pain she went through made my pain increase. School was supposed to be my escape but it made things worse. My body felt like shutting down but it never did. I couldn't close my eyes at night because I was afraid I would see her die in my dreams. I felt like there was no purpose in life. If my mom passed, I would make sure I was right behind her. After seeing her one night at her worst, I broke down right there in the hospital. My legs became weak, my stomach cringed tight, my arms felt like they were falling off, my head felt like it was going to burst into tiny pieces due to the pressure, and my heart was nowhere to be found. It had vanished from my flesh. With my head down, I walked out of the hospital, straight outside into the cold night air, until a hard rock body slammed into my body with arms embraced around me like they were locked. I didn't look to see who it was because a hug was all I needed. After a while, I realized it was my dear friend, who I like to call my "lifeguider." Any time I have a problem she's just a phone call away and she knows exactly what to say. We talked for an hour outside the hospital, and she said, "I was on my way home and I was just about to call you and as I passed by the hospital, something made me stop to check on you. I didn't know exactly where your mom was located in the hospital, but somehow I knew I would find you." The next two months felt like two years. My dad was under a great deal of stress ten times more than I was. I'd never seen him like that and I knew this wasn't him. I was used to the pain by now. I wouldn't cry anymore because I didn't think my body could. I never ate because I was never hungry anymore. Like I said, my body shut down-things I did before were no more. Every day, I repeated the same process of waiting for time to pass and seeing what the future had in store for me. Finally, after those two months, my mom returned home. It felt like the day of redemption and a weight had been lifted off my whole body. In a week, she had returned to her normal self again. It was as if God was her and she couldn't be hurt anymore. Karen shares her own story about friends made through the APF In Touch network here.
Remember.Research is the key to your cure!
Why join the APF In-Touch
Friday - May 17, 2013 @ 18:24:39
Join APF In Touch
Because porphyria is a rare disease (defined as affecting fewer than 200,000 sufferers in the U.S.), many newly diagnosed patients have never even heard of the condition before, let alone met someone else who suffers from it. We created the APF In Touch network to meet this need. APF membership includes access to the In Touch network, through which members can contact others around the country who are dealing with porphyria. Some members form lasting friendships via email, telephone or old-fashioned letters. Others prefer to reach out to members in their region and organize face-to-face get-togethers. If you are seeking support and fellowship, or are willing to be there for others who are dealing with porphyria, please fill out and send in the In Touch consent form to our address below. For more information on the APF In Touch network, contact Yvette at the APF office: 866-APF-3635 or 713-266-9617. American Porphyria Foundation 4900 Woodway, Suite 780 Houston, TX 77056
What the In Touch network has done for me:
I want to share my experience with the In Touch network provided to us by the Foundation. I was diagnosed with AIP after 18 months of symptoms. You know the severe abdominal and back pains with fatigue and nausea. You all know the drill. The scariest part was the rarity of this disease. Every doctor tells you they're not that familiar with it, and very little was actually known about it. People look blankly at you when you try to explain how you feel. I don't have to elaborate to you all that also have it. So I decided to communicate with someone else that had this illness. This was back in 2001, the time before the wonderful website that we are so blessed with now. So I opened the newsletter and looked at the names before me. I knew that I wanted someone that also had AIP. So I closed my eyes and asked God to help me chose the right one. I opened my eyes and there she was. Lori Brown from Madison, Alabama. I am from Arkansas so she was geographically close to me. I emailed her and introduced myself to her, telling her all of my experiences so far and asked if she would like to share "war stories." She emailed back and was more than happy to do just that. So over the next 7 years Lori and I battled porphyria together. After a while Lori and I began calling each other on the telephone. Some of our conversations lasted for two hours! We discussed how the disease affected our marriages, children and our lives in general. I don't know if it was misery loves company but I can tell you she helped me so much. To have someone who understands what you are going through is great. I didn't feel alone. On October 16, 2008 Lori Brown from Madison, Alabama passed away. The battle with porphyria is over. She is free. I never got the privilege of seeing her face or giving her a hug. But she was one of my best friends. So if you are thinking about getting in touch with someone and just haven't done it yet I encourage you to find yourself a Lori too. Find several. I have others as well: Rose, Mira, Judy, Jennifer and Troy. Or attend a meeting scheduled near you. Or reach out and host one yourself. I can assure you it will be a fulfilling experience. Karen Eubanks Conway, AR
Remember.Research is the key to your cure!
A Story about Michelle Bridges and AIP
Friday - May 17, 2013 @ 18:21:50
Michelle Bridges
Type of Porphyria:
Acute Intermittent Porphyria (AIP)
I spent my whole life with unexplained symptoms. Sometimes my legs would give out, and I would have back pain, abdominal pain, slurred speech, difficulties walking and so forth. When I was 16, doctors found a mass in my brain. After removing what they could, all my health problems were blamed on post surgical changes. In 2005, the doctors began to wonder about other causes. I was sent to see a gastroenterologist and diagnosed with pancreatitis. But there was no explanation for my abdominal pains that would come out of nowhere and then disappear. The doctors decided that is was due to a problem with my digestion and cut part of my bile duct. However, I landed back in the hospital with pancreatitis. Then nothing happened for about eight months. At the end of July 2006, I began to have problems again. They put me on Reglan with the intention of running more tests and after about a week, I woke up feeling bizarre. I was in a haze and unable to function. I had called a friend and asked her to take me to the hospital. I turned to walk down the hall towards my bedroom so I could lie down, but my legs would not move. I remember standing there thinking you bend the knee and extend the leg. By the time I had dragged myself down the hall, my arms wouldn't cooperate and I fell over. When the paramedics got the house I swear I asked if I was having a stroke. My son says I just lay there with my tongue hanging out, in and out of consciousness and seizure activity. I don't remember. The ER released me to my husband with the diagnosis allergic reaction. The following day I could not speak. Again, I went to the ER, but this time it was to a different hospital, one covered through our insurance. The doctor told my husband I was being over-medicated, and then a student at the hospital noticed the color of my urine and suggested to the doctor that my condition might be porphyria. She was correct! I don't remember anything from the end of 2006 to 2008. Treatment for my symptoms made some things worse. I had been active in my church and homeschooled other peoples children as well as my own, but I had to stop educating others and withdrew from some activities at church. We have had a hard time finding doctors who will treat me. This disease is rare and doctors aren't experienced with it. With my new oncologists gentle touch and the support of the staff at our new hospital, I have become more active. I am not spending as much time in the hospital, and I still homeschool my children, write curriculums and resource guides, and do crafts for craft fairs and whatever else I can to support the church and help others. I do all of these activities from my bed because I am too weak and have too much pain to leave the bedroom for long stretches and I get sick so easily. But I do like to have some level of activity in my life and so I try to contribute where I can while being careful of my health.
Remember.Research is the key to your cure!
Treatment Options
Friday - May 17, 2013 @ 18:18:23
Treatment Options
The American Porphyria Foundation promotes comprehensive care necessary for treating individuals with Porphyria. Although there is no cure for porphyria, there is treatment available for each type of the disease.
In this section of our website you'll find detailed information on Panhematin for acute porphyria (AIP, VP, HCP or ADP) and Lumitene for Erythropoietic Protoporphyria (EPP), tips on finding a local doctor and building a good working relationship with your doctor. Treatment for each of these diseases involves more than a single medication. Please see the disease descriptions for additional information.
Panhematin is a treatment for the acute porphyrias manufactured by Lundbeck Inc. in Deerfield, IL. It is a lyophilized form of alkaline heme that has to be reconstituted immediately prior to administration. Panhematin should be infused into a large peripheral vein. A large central line or port may be used, if available.
Doctors administer Panhematin to correct heme deficiency in the liver and repress production of porphyrin precursors. Panhematin almost always normalizes porphyrin and porphyrin precursor values. Three to four mg/kg of Panhematin given once daily for four days early in an attack produces a highly beneficial effect in most patients. Commonly noted are decreases in pulse rate, blood pressure, abdominal pain, as well as decreased levels of urinary porphobilinogen (PBG). These effects can occur within a day.
Panhematin is the only commercially available heme therapy in the United States. (Heme arginate is another preparation, but is only available outside of the U.S.) While a high carbohydrate diet is recommended for patients with porphyria, it is not regarded as highly effective by itself. Intravenous glucose therapy is a treatment option for mild attacks. When heme therapy was introduced as a treatment, it was recommended that it be initiated only after several days of glucose therapy was unsuccessful.
Today, physicians experienced in treating patients with attacks of porphyria recommend early use of Panhematin rather than waiting to see if glucose alone will be of decisive help.
Remember.Research is the key to your cure!
Clinical Studies: What's in It for You?
Wednesday - May 15, 2013 @ 23:21:47
Clinical Studies:
Whats in It for You?
All porphyria patients and their families can contribute to
medical knowledge of these diseases by volunteering for research.
Each of the five Porphyria Clinical Research Consortium
centers is recruiting patient volunteers with all types of
porphyria. Participation could include treatment trials, or simply
visiting a Consortium clinic.
I have been lucky enough to take part in two clinical studies
since my diagnosis with AIP in 1995. For me the most rewarding
part of each project was the one-on-one time spent
with a porphyria expert. As part of each study I was examined
by, and discussed my history with, a doctor who had
spent an entire career studying and treating the porphyrias.
From a purely selfish point of view, I found it comforting to receive
feedback on my experience with AIP, and advice about
future treatment, from physicians who have seen more than a
handful of cases. While I have always liked the doctors who
care for me at my local hospital, speaking with an expert
gave me added confidence that I am following the best
course of treatment for me.
There is also the greater good to be served by taking part in
a study. Patients who volunteer for clinical research can be
proud to know that they are adding to medical knowledge
about porphyria, making it possible for other patients to receive
better care. Understanding that porphyria is a family
disease makes this easy for anyone to relate to.
Mira Geffner
Remember.Research is the key to your cure!
Sensitivity & Specificity of tests for Porphyria
Wednesday - May 15, 2013 @ 23:19:00
Sensitivity & specificity of tests for Porphyria
Sensitivity is a feature of many of the diagnostic tests for porphyrias, especially when they are done at or near the time of symptoms. Tests that are sensitive for diagnosis of active porphyrias are almost always abnormal when symptoms of Porphyria are present. But the tests vary in specificity, meaning that some of the tests (those with lower specificity) are abnormal in other diseases. In choosing a test to screen for a disease that is not only uncommon but also causes symptoms that mimic more common diseases, it is obviously important to choose a test that is both sensitive and specific. Fortunately, some tests for Porphyria have both of these features. With such tests, it should always be possible to determine if symptoms might be due to one of the porphyrias.
Table 1. Diseases due to deficiencies of specific enzymes of the heme biosynthetic pathway
The enzymes and their intermediates (substrates and products) are shown in sequence. Some intermediates are porphyrinogens (reduced porphyrins); these are excreted and measured mostly as oxidized porphyrins (click on any of the yellow-highlighted enzyme names to determine if the substances should be measured in blood, urine or feces). A deficiency of the first enzyme, ALAS, causes a type of anemia rather than a Porphyria. (Uroporphyrinogen I synthase is an obsolete term for PBGD and is not shown in the Table.)
Porphyria should be suspected quite frequently, because the symptoms that suggest the diagnosis are common. If a diagnosis of Porphyria is not made promptly, serious consequences to the patient may follow. But more often than not, laboratory testing will show that the patient does not have Porphyria, because other diseases with symptoms that mimic Porphyria are much more common. An effective approach to laboratory testing is one that does not often miss the diagnosis and also does not often incorrectly suggest that Porphyria is present.
Remember.Research is the key to your cure!
Misinterpretation of test results
Wednesday - May 15, 2013 @ 23:17:23
Misinterpretation of test results
Diagnosis of Porphyria is often delayed, and it has become widely recognized that physicians should maintain a high index of suspicion for these conditions. It is less widely appreciated that incorrect diagnoses of Porphyria are common in patients with symptoms due to other diseases. Therefore, in patients with a past history of Porphyria, it is important to review the laboratory data that were the basis for the original diagnosis. Further testing may be necessary if the diagnosis was not adequately documented. Incorrect diagnoses of Porphyria can occur in patients having minimal abnormalities in laboratory tests, such as small elevations in urinary porphyrins or porphyrin precursors that in fact have little or no diagnostic significance. Incorrect diagnoses are less likely if reliance is placed on a few first-line tests in most clinical situations, as described above. Overuse and over interpretation of minor abnormalities in results of second-line tests including erythrocyte PBGD, other enzyme assays, and fractionation of urinary and fecal porphyrins, account for many incorrect diagnoses of Porphyria. AT PRESENT LABCORP & QUEST ARE NOT RECOMMENDED FOR EPP TESTING. Remember.Research is the key to your cure!
U.S. Porphyria labs
Monday - May 13, 2013 @ 22:26:31
There has been many questions as to where Porphyria Testing can be done. The American Porphyria Foundation can help you. For additional information please visit: www.porphyriafoundation.com
There are only a few laboratories in the United States that can perform the complex analysis to diagnose Porphyria. The laboratories listed with a ** are overseen by a Porphyria expert who can consult with your physician about your test results. It is always best to have your doctor's office call the laboratory before sending samples to verify collection and shipping instructions.
University of Texas Medical Branch** Porphyria Center Dr. Karl Anderson RT-J 09 Ewing Hall Galveston, TX 77550 (409) 772-4661 ARUP Laboratories** University of Utah 500 Chipeta Way Salt Lake City, UT 84108 (801) 583-2787 Fairview University Diagnostic Laboratories University Campus, Mayo Bldg., Room D-293 420 Delaware Street SE (UH-198) Minneapolis, MN 55455 (612)-273-7838 Please note: This lab does urine tests on site; blood and stool samples are sent out to the University of Texas, Galveston Porphyria Laboratory for testing and interpretation. Mount Sinai Medical Center** Department of Human Genetics Dana Doheny, MS, CGC, Genetic Counselor Porphyria DNA Testing Laboratory Department of Human Genetics & Genomic Sciences Mount Sinai School of Medicine 1425 Madison Avenue, Room 14-74, Box 1498 New York, NY 10029-6574 Tel: (212) 659-6779 Email: porphyria@mssm.edu DNA testing for six porphyrias: AIP, HCP, VP, f-PCT, EPP, CEP Quest Diagnostics 33608 Ortega Highway San Juan Capistrano, CA 92690 (800) 642-4657 AT PRESENT LABCORP & QUEST ARE NOT RECOMMENDED FOR EPP TESTING Mayo Medical Laboratories Tel: (800) 533-1710 or (507) 266-2888 Fax: (507) 266-2888 Please note: The physician or hospital ordering the tests should phone ahead to the laboratory before ordering tests or shipping samples. Telephone consultation is provided to health care professionals only. Direct patient consultation is not provided over the telephone.
Remember.Research is the key to your cure!
A Lesson in Humility
Monday - May 13, 2013 @ 22:17:41
If you can start the day without caffeine, If you can get going without pep pills, If you can always be cheerful, ignoring aches and pains, If you can resist complaining and boring people with your troubles, If you can eat the same food every day and be grateful for it, If you can understand when your loved ones are to busy to give you any time, If you can overlook it when those you love take it out on you, when through no fault of yours, something goes wrong, If you can ignore a friend's limited education and never correct him, If you can resist treating a rich friend better than a poor friend, If you can face the world without lies and deceit, If you can conquer tension without medical help, If you can relax without liquor, If you can say honestly that deep in your heart you have no prejudice against creed, color or politics, Then my friend, you are almost as good as your dog. What words to think about! Anonymous
As the year comes to a close, my wish is that each of us will be able to take some time to reflect on 2012 and look ahead with enthusiasm to 2013, despite whatever challenges we may anticipate encountering in the new year. As one cycle ends and another begins, we have an opportunity to make choices for the new year, and I hope that each of us is able to commit to putting into practice steps that will enable us to relate to stress more masterfully and, in so doing, to live more fully. As I continue to outline the main tenets of the nine natural steps in this blog series, I would like to close 2012 with one of the most practical of the steps: exercise. Specifically, I want to talk about walking. Making a commitment to introducing daily exercise into your life in 2013 is a tremendously beneficial decision to make. Daily walking was one of the most important components in my learning to master stress and recovering from my breakdown. Walking is the most natural form of exercise for humans; our evolutionary makeup is built for it. This is why I am a strong advocate of a brisk, uninterrupted daily walk for at least one hour. Although I support and encourage any form of exercise that an individual finds enjoyable and useful, I strongly recommend embracing the following walking program for optimal health and to achieve maximum benefit from the nine steps.
As the father of modern medicine, Hippocrates, said, Walking is mans best medicine. Although I tried many different forms of exercise while I was rebuilding myself, such as running, cycling, and swimming, after much research and trial and error, Ive concluded that walking is the most effective and natural mode of exercise. I was first motivated to study the benefits of walking while observing my grandmothers transformation after the death of her husband, when she adopted a daily walking practice. She had been overweight for as long as I could remember. I was impressed, however, by her increased vitality and the amount of weight she lost from her daily walks. She ended up maintaining excellent health right up until her death at the age of ninety-six. Having now experienced the benefits of daily walking myself, I am sure that this component of her lifestyle contributed greatly to her robust health.
The human body was clearly not built to fly or swim, as is evident when comparing our makeup to that of a bird or a fish. On closer examination, it also is apparent that we were not built to jog or run long distances, which places our joints under a high amount of strain. While the origins of running, for humans, lie in the fight-or-flight mode, running has grown in popularity as a form of exercise; more than 425,000 Americans ran a marathon in 2010, up 20 percent from the year 2000. While it clearly requires dedication and the building of a strong, healthy body to run a marathon, the New York Times reports that 90 percent of people who train for a marathon sustain some type of injury in the process. The benefits of running and any other form of exercise must be weighed against the costs, and it is up to each individual to decide what suits his or her needs. Having been a long-distance runner as well as a hurdler and sprinter at school and having had a continued interest in exercise and sport all my life, I am aware of the benefits and costs of different forms of exercise. I have thoroughly researched and tested various modes against one another.
Daily walking to promote health is going back to basics, supporting the body in the most natural and effective way. Consider other forms of exercise and how there is a limit to how long one can continue for at a time, whereas, when it comes to walking, people are able to walk comfortably for hours at a time, further evidence of walking being the optimal exercise for sustainable enjoyment and benefits. Just as Chinese healers utilize nerve endings in the feet to promote overall wellness, walking stimulates those same 7,200 nerve endings, helping to balance your entire system. Longevity studies often reveal that those living the longest tend to walk daily as a form of exercise, well into their golden years. The simplest and most effective way to implement an effective and sustainable exercise routine is to walk briskly for sixty to eighty minutes every day, on your own, without interruption.
This kind of walk doesnt allow for any distractions such as talking with friends, using a cell phone, or listening to music, and it is certainly not compatible with watching TV on a treadmill. Any such activities must take place outside of your primary walking time and should not steal away from time to focus and reflect within yourself. Later, once your body has been strengthened and cleansed by your walking program, you may choose to walk for one hour, three to four times a week.
If possible, immerse yourself in the natural environment, whether walking on grass, on sand, in a forest, by a riverbank, or in a park. The undulating surface of the natural environment is stimulating and invigorating for the body and the central nervous system. Nature is what the body has developed to expect. Your walk should always be enjoyed outside so that you can breathe the fresh air and embrace the natural environment in natural light. This is indeed a joy to be treasured in life. Additionally, sunlight is an irreplaceable source of vitamin D, which is produced by our bodies as a response to our skins exposure to the sun. The reality is that many of us do not live near a beach or a forest, so use a nearby park or sidewalk when needed, and enjoy your walk. Even in the concrete jungle of Manhattan, I have walked consistently through summer and winter between six a.m. and seven a.m. Heading out early avoids traffic, and despite the urban background of noise and skyscrapers, it still offers much more than a treadmill in an enclosed gym. Dont let a little rain or cold deter you from your walk; dress appropriately for the conditions, and do your best to walk outside whenever you can. Even though I miss walking barefoot on the beaches of Sydney, Santa Monica, and Auckland, I still make the most of my surroundings by heading straight for Central Park every morning, enjoying every moment of this alone-time and the serotonin boost that this natural form of exercise provides.
The ideal time to exercise is early in the morning. I encourage putting aside this time to begin your day, which prepares you for the rest of the activity to come and allows you time for reflection. Ensure that your sixty to eighty minutes of walking is continuous, as pauses will limit some of the benefits and the stimulation that the exercise provides. Your morning walk should be brisk, close to your maximum speed, with your elbows bent and hands swinging up to eye level if you are able. This gives you comprehensive physical exercise as you engage both the upper and lower body; the activity of walking in such a way works not only the muscles of the legs but the entire body, including the hips, spine, shoulders, abdomen, and arms. The head should remain level, with your eyes taking in your surroundings or focused on where you are heading but not gazing downward as if you are low on energy.
Introducing a brisk walk that adheres to the above guidelines into your daily routine is a highly effective way of conditioning the body and mind while also releasing stress. As we prepare for the activity of a new year, I hope you will take some time to rest, reflect, and decide on your true health and well-being priorities for 2013.
Remember.Research is the key to your cure!
Marlene Breeze & AIP
Thursday - May 9, 2013 @ 14:43:51
Marlene Brezee
Type of Porphyria:
Acute Intermittent Porphyria (AIP)
It's hard to believe it's been thirty years since my diagnosis. I thought life as I had known it was over. I had a loving husband, two wonderful children and nothing really bad had ever happened to me. I found out at the age of thirty that I was going to have another child. Everything went fairly well up until about five months into the pregnancy. I began to have abdominal pains. The pain would come and go. I would go into the hospital, stay a while, be diagnosed with false labor and given medication. In and out- In and out. The pain, however, became increasingly worse and was accompanied by nausea and vomiting. I also had a strange thing start happening. My urine turned tea colored. Meanwhile, back into the hospital they were trying to discover what was wrong and gave me more medication, another consult with another doctor, and again the diagnosis of false labor. My doctor decided to try an old remedy of using an alcohol I.V. to stop the false labor; I was now in a lot of distress and my moaning and groaning could be heard outside of my room. The other patients began asking what was wrong with that woman? Things then went from bad to worse, and I was sent by ambulance to the University Of Michigan Hospital in Ann Arbor. It was a frightening time in my life. It's very scary when you are so very ill, and the doctors can't find out why. My family and friends were praying so hard for me. My husband was such a comfort and rock when with me but told me later how he had sat out in the parking lot crying and praying when things seemed so dark. God's timing is always perfect. It doesn't, however, mean that He answers as quickly as we would like. At the U of M Hospital they immediately took all medications away from me, including the pain meds. I now felt desperate. I begged them and my family to have them do surgery to see what was wrong. I knew if they would just go in and look, they would see the problem. The doctors had discussed a possible bowel problem but they really didn't know. As I say, God's timing was prefect and oh so merciful. In a few hours I was to have an exploratory laparoscope. At five months my baby would be at great risk. How I remember the words from the two doctors standing by me as they looked down at my catheter. Those few words would change my life. "I don't like the color of the urine; The test is simple enough, do it;" The test came back positive for porphobilinogen and subsequent tests were positive for porphobilinogen. All surgery was now stopped and the diagnosis of Acute Intermittent Porphyria was given. My local doctor told me later, I was so close. I kept thinking, "What causes abdominal pain and red urine? " ; He couldn't remember, but you see, God knew the timing wasn't right. Perhaps we all had more to learn. As I was to find out later, Porphyria can be called the "little Imitator," as it can mimic so many other conditionsThe doctors realized that the very meds that had been given to help me were in fact making my symptoms worse. My life as I had known it thirty years ago was not over for me. The baby, even though he was born two months prematurely, is now six feet three inches tall, married and in full time Christian work. I have told him how God protected him in his mothers womb. At times I tend to worry over him, as I do with all my children, but I like to remind myself that God loves him more than I ever could. I cannot say that I have never been bothered with Porphyria again, but never for that long. I have had some episodes of severe nausea and vomiting especially after surgery or colonoscopies, and I did have a couple episodes two or three years ago that were suspect. The one started out with my head feeling whoozy, and I started to feel nauseous. I have migraine headaches, so I wasn't sure what was happening. I went to get up and walk and was so tired I sat right on the floor for awhile. I was able to get into the car but while getting to the doctor's office my legs and arms felt very strange and very weak. The only releif I could get was to hang my head as close to the car floor as I could get it. By the time I got to the doctor's office, I was so weak that the doctor described it as flacid. I was sent by ambulance from there to the ER. I received one IV glucose push in the doctor's office by the paramedic and one or two more at the hospital. I responded very well. Late that evening they started a 24 hour urine test. For whatever reason the test did not show positive. This is still a puzzle to me. I had been taking a drug that my doctor felt that may have been the reason I got into trouble. She says she won't ever prescribe another similar one for me. At age 61 looking back to the day of diagnosis, I realize I have done very well. When I feel good, which is most of the time, I feel so good that it is actually hard to imagine being sick.
Remember.Research is the key to your cure!
Read, Think, Learn and Act Quickly
Thursday - May 9, 2013 @ 11:55:46
I wanted to take just a few moments to say how thankful I am for the American Porphyria Foundation. They provide so many things for us. Even though I have AIP, I see so many of you that have EPP, have gone through the trials and could see a real difference. Just when youre not feeling good what do you do to protect yourself? I hope that you can get the courage to write how you feel about how you have benefited already from your experience; how you need a drug so you can live your life to the full. Thinking back about how the APF has helped many of you from diagnosis, doctors and treatments, can you pay it forward?
When I have AIP attacks it is one of the most miserable things to endure, when I have the opportunity to do my part in trials, learning, education, writing letters to express how I feel about having a rare disease and how a drug can make me feel better, I speak I write I tell anyone who will listen to me why I need support, approval for research and new medications. So I encourage each and everyone one of you to support each other, get your families, friends to express how you need an approved treatment here in the United States. Its made so much progress all around the world. Please send your letter ASAP.
To the: American Porphyria Foundation
4900 Woodway, Suite 780, Houston, TX 77056. Toll free: 1.866.APF.3635.
Remember.Research is the key to your cure!
Cook Brothers and family promote Awareness Week.
Thursday - May 9, 2013 @ 09:52:17
Cook Brothers and family promote Awareness Week.
The Cook brothers, Cason (11) and Caul (10) have started a Porphyria Awareness Week HAT DAY tradition in their home town of Vernon, Texas. Both brothers have EPP and have set a great example about enhancing awareness of the disease in their own local area. The boys wanted to raise money for the APF, too, so they asked the school board if they could do an awareness event and raise funds for the APF by hosting HAT DAY where everyone at their schools who wanted to participate could wear a hat in honor of the brothers and bring one dollar for the APF. The students loved the idea. It also gave Cason and Caul a chance to teach their school mates about porphyria, especially EPP. The boys explained about not being able to be in the sun and how it affects them, thus giving their friends a greater understanding of the severity and complexity of EPP.
Cook Family: L-R, Caul, Cason, Lee Ann, Chris
Also, employees at many businesses could do the same by bringing a dollar and wearing a hat every day of Awareness Week. Their whole community got involved and businesses even contributed by giving discounts. The Cook family also hosted another successful fundraising and awareness event at their church. This was such a wonderful and fun way to promote awareness and raise fund for physician education.
Rememberâ?¦..Research is the key to your cure!
Clinuvel programs and SCENESSE
Thursday - May 9, 2013 @ 09:42:16
The technology behind Clinuvels lead drug, SCENESSE (afamelanotide), has been in research and development since the 1980s when a small team of scientists set out to investigate methods of preventing skin cancer in humans. Clinuvel licensed this technology and has spent over A$20million optimising the chemistry of afamelanotide (the active ingredient in SCENESSE) and developing a proprietary, controlled-release implant formulation.
Since late 2005, Clinuvel has focused on developing SCENESSE as a dermatological drug for individuals at greatest risk from visible and ultraviolet (UV) light. The company has a particular focus on diseases where no existing preventative treatment exists.
Clinuvel commenced a clinical program in 2006 which focused on the rare diseaseerythropoietic protoporphyria (EPP), a metabolic disorder which causes painful burning reactions under the skin after even brief exposure to sunlight. The goal of Clinuvels EPP program is to prove that SCENESSE can provide patients with EPP protection from sunlight by reducing the incidence and severity of EPP reactions. The ultimate objective is to provide a better quality of life for patients. Since the start of the EPP program, the company has involved more than 250 individuals with EPP in its global clinical trials. Between 2005 and today, clinical programs have also been conducted for individuals diagnosed with a range of disorders, includingpolymorphous light eruption,solar urticariaandorgan transplant recipientswho are susceptible to an extremely high rate of skin cancers.
In late 2009, Clinuvel announced that it had expanded its pipeline to include a second drug candidate, namedCUV9900. Based on the same technology as SCENESSE, CUV9900 is still in early stage development.
2010 was a pivotal year for Clinuvel. In May 2010, SCENESSE became the first dermatological drug listed under theItalian 648/96 law, prior to its formal approval anywhere in the world. This listing allows Italian physicians to prescribe SCENESSE to individuals with EPP with the cost of the drug reimbursed by the Italian National Health System (Sistema Sanitario Nazionale, SSN).
Later in 2010, Clinuvel also announced that it would expand its program for SCENESSE to investigate the drugs ability to repigment skin in the common pigmentation disordervitiligo. Following regulatory and ethical approvals, Clinuvels International SCENESSE Pilot Repigmentation Evaluation (INSPIRE) program commenced patient recruitment in 2011.
In February 2012 Clinuvel lodged its first marketing authorisation application for SCENESSE for EPP with the European Medicines Agency.
As of April 2012, more than 620 individuals have been administered afamelanotide in Clinuvels clinical trials program. To date, the drug has maintained a good safety profile in clinical trials.
Rememberâ?¦.. Research is the key to your cure!
SCENESSE data to be presented at American Academy of Dermatology, San Gallicano Rare Disease conferences-US Info
Tuesday - May 7, 2013 @ 18:44:16
Company Announcement SCENESSE data to be presented at American Academy of Dermatology, San Gallicano Rare Disease conferences Vitiligo and erythropoietic protoporphyria (EPP) programs to feature at leading academic meetings Melbourne, Australia and Baar, Switzerland, March 1, 2013 Clinuvel Pharmaceuticals Limited (ASX: CUV; XETRADAX: UR9; ADR: CLVLY) today announced that data from its clinical studies of the novel drug SCENESSE (afamelanotide 16mg implant) in vitiligo and erythropoietic protoporphyria (EPP) will be presented at two international academic conferences this week. Results and clinical observations from the Phase IIa study of SCENESSE in vitiligo (CUV102) will be presented at the Vitiligo Working Group meeting, accompanying the American Academy of Dermatology AAD meeting in Miami. An abstract featuring the CUV102 study will also be presented to the AAD Residents and Fellows Symposium at the main AAD meeting. Experiences of the use of SCENESSE as a photoprotective in the rare disease EPP in Italy will be discussed at the San Gallicano Conference on Rare diseases. This presentation will focus on the experiences with the drug in both clinical trials and commercial use in Italy. End References American Academy of Dermatology, Miami Isedeh P, Agbai O, Lim HW & Hamzavi I (2013). A Proof of Concept Study to Compare the Efficacy of Subcutaneous Afamelanotide Implants and NarrowBand Ultraviolet B (NBUVB) Phototherapy versus NBUVB Alone in the Treatment of Nonsegmental Vitiligo. Vitiligo Working Group Meeting, Miami, February 28. Agbai O, Lim HW & Hamzavi I (2013). A Proof of Concept Study to Compare the Efficacy and Safety of Subcutaneous, Bioresorbable Afamelanotide Implants and NarrowBand Ultraviolet B (NBUVB) Light versus NarrowBand Ultraviolet B (NBUVB) Light Alone in the Treatment of Nonsegmental Vitiligo. American Academy of Dermatology Meeting Residents & Fellows Symposium, Miami, March 3. Rare Disease Conference, Rome Biolcati, G Terapia EPP. Le Malattie Rare AllInstituto San Gallicano, Rome, March 1. About SCENESSE (afamelanotide) SCENESSE is a firstinclass therapeutic being developed by Clinuvel, with the generic name (or INN) afamelanotide. An analogue of αMSH, afamelanotide is a linear peptide which activates eumelanin of the skin, the dark pigment which is known to provide photoprotective properties (offering skin protection against light and UV radiation). SCENESSE is administered underneath the skin as a dissolvable implant approximately the size of a grain of rice. For more information on SCENESSE go to http://www.clinuvel.com/en/scenesse. SCENESSE is a registered trademark of Clinuvel Pharmaceuticals Ltd. About Clinuvel Pharmaceuticals Limited Clinuvel Pharmaceuticals Ltd (ASX: CUV; XETRADAX: UR9; ADR: CLVLY) is a global biopharmaceutical company focused on developing drugs for the treatment of a range of severe skin disorders. With its unique expertise in understanding the interaction of light and human skin, the company has identified three groups of patients with a clinical need for photoprotection and another group with a need for repigmentation. These patient groups range in size from 10,000 to 45 million. Clinuvels lead compound, SCENESSE (afamelanotide), a firstinclass drug targeting erythropoietic protoporphyria (EPP), has completed Phase II and III trials in the US and Europe. In February 2012 SCENESSE was filed for review by the European Medicines Agency for EPP. A confirmatory six month Phase III US EPP trial commenced in May 2012. Presently, there is no known effective treatment for EPP and SCENESSE has been granted orphan drug status. Based in Melbourne, Australia, Clinuvel has operations in Europe and the US. For more information go to http://www.clinuvel.com. Investor contacts: Australia: Clinuvel Pharmaceuticals Limited, T: +61 3 9660 4900 Europe: Clinuvel AG, T: +41 41 767 45 45 E: investorrelations@clinuvel.com Media contacts: Lachlan Hay Clinuvel AG Baar, Switzerland T: +41 41 767 45 45 Lachlan.Hay@clinuvel.com Clinuvel is an Australian biopharmaceutical company focussed on developing its photoprotective drug, SCENESSE (afamelanotide) for a range of UVrelated skin disorders resulting from exposure of the skin to harmful UV radiation. Pharmaceutical research and development involves long lead times and significant risks. Therefore, while all reasonable efforts have been made by Clinuvel to ensure that there is a reasonable basis for all statements made in this document that relate to prospective events or developments (forwardlooking statements), investors should note the following: � actual results may and often will differ materially from these forwardlooking statements; � no assurances can be given by Clinuvel that any stated objectives, outcomes or timeframes in respect of its development programme for SCENESSE can or will be achieved; � no assurances can be given by Clinuvel that, even if its development programme for SCENESSE is successful, it will obtain regulatory approval for its pharmaceutical products or that such products, if approved for use, will be successful in the market place Level 14 / 190 Queen Street T +61 3 9660 4900 www.clinuvel.com Melbourne, Victoria 3000 F +61 3 9660 4999 Australia
Rememberâ?¦.. Research is the key to your cure!
Inspirational quote
Tuesday - May 7, 2013 @ 17:31:42
Here's a late night inspirational quote for those of us dealing with illness or uncertainty in our future. Stay strong, everyone - and let's make the upcoming week a great one!
Rememberâ?¦.. Research is the key to your cure!
Top Tips for a Healthy Summer
Tuesday - May 7, 2013 @ 11:29:52
Top Tips for a Healthy Summer Vacation
Put safety first to ensure a healthy vacation this summer, both while you're away and when you're lounging in your own backyard.
Take a Smart Approach to Summer Safety
Ahhhhâ?¦summertime. Time to relax and enjoy. But it also means it's time to take precautions against the sun's harmful rays and excessive heat. Whether you spend your summer vacation in a tropical area, at home, or at the beach or a lake house, keep safety first. Here are the season's top tips for staying healthy during an active summer, home or away.
Drink Up the H2O
For a healthy summer, drink plenty of water. "Avoid caffeinated and alcoholic beverages, which can cause dehydration," says Jessica Bartfield, MD, a specialist in internal medicine and bariatrics at the Loyola Center for Metabolic Surgery & Bariatric Care in Melrose Park, Ill. "Fresh seasonal fruits and vegetables are also a great way to keep you hydrated, and they also provide essential vitamins and minerals." Summer safety double-check: You may be dehydrated if your skin tents (when you pinch your skin, it forms a ridge) or your urine is dark.
Exercise With Caution
Especially when enjoying an active summer, make sure you drink more water than usual, Dr. Bartfield advises. If you exercise outdoors during a heat wave, do it early in the morning when temperatures are lower and the sun is less intense. Hot temperatures can also bring on painful muscle spasms called heat cramps. "When you drink lots of water but don't replace salt that's lost through perspiration, muscles can cramp up," she says. "Try drinking an electrolyte solution, such as a non-caffeinated sports drink, to ease cramps."
Breathe Easy
Deepti Shivakumar, MD, a family physician with Loyola University Health System and Gottlieb Memorial Hospital in Melrose Park, Ill., warns that if you're older, have chronic medical conditions, or have a sensitive respiratory system, you're more prone to breathing difficulties in high heat and humidity. To ensure ahealthy summer, he advises staying in air conditioning and taking cool showers. Wear loose cotton clothing, too, as a comfortable summer-safety step.
For all the Epp, CEp, PCT, HCP, VP Take more time to be in the shade.
Wear Shades
Don't forget about keeping your eyes in good health during an active summer. For summer safety, wear sunglasses that protect not only the lens, cornea, and other parts of your eye, but the eyelid and surrounding skin. "Choose sunglasses that block 99 percent to 100 percent of both UVA and UVB rays, and select a large lens or wraparound style for best coverage," Dr. Shivakumar says. "Some contact lenses offer UV protection, but they don't cover the entire sensitive eye area, so you should still wear sunglasses."
Don't Get a "Base" Tan
Put summer safety first when it comes to your skin. There's no such thing as a "base" tan, and getting one will certainly not protect you from the sun's UV rays, says Richard Bezozo, MD, president of MoleSafe in Millburn, N.J., a digital imaging technology that tests moles for melanoma. According to the U.S. Centers for Disease Control and Prevention, up to 90 percent of melanomas, the most deadly form of skin cancer, are caused by exposure to UV light radiation, which comes from the sun, tanning beds, and sunlamps. When in the sun, whether you're having an active summer or just taking a walk, be sure to wear sunscreen.
Minimize Sun Exposure
Have a healthy vacation by avoiding the sun during its most powerful hours. The sun's UV rays are the strongest from 10 a.m. to 4 p.m. Instead, go shopping, have lunch, or partake in other fun vacation festivities, Dr. Bezozo advises. If you want to hang out at the beach or enjoy a daylounging at the pool, consider renting a cabana or bringing a large umbrella to help shade you from the sun for prolonged hours.
Protect Your Skin Every Day
Another way to keep your skin protected is to wear a water-resistant sunscreen with an SPF of at least 30. For summer safety, apply the sunscreen 20 minutes beforegoing outdoors and reapply every one-and-a-half to two hours. "Don't forget that you need sunscreen even on cloudy days," Bezozo says. Approximately 50 percent to 80 percent of UV rays penetrate through the clouds. You can also reduce your risk of skin cancer by wearing a hat, UV-blocking sunglasses, lip balm with an SPF, and protective clothing like long sleeves and pants.
Beware of Critters
Bugs thrive in warm climates. When you're having an active summer outdoors, protect yourself from bites, stings, and infections by wearing an insect repellent that contains the common ingredient N,N-Diethyl-meta-toluamide, or DEET, (30 percent to 50 percent) or picaridin (up to 15 percent). This is a must for summer safety whenever you're outdoors in areas where disease-carrying insects are active, even in your own backyard, Shivakumar says.
Rememberâ?¦.. Research is the key to your cure!
Clara Hauke EPP!
Monday - May 6, 2013 @ 16:37:51
Clara Hauke
Type of Porphyria:
Erythropoietic Protoporphyria (EPP)
Im 18 years old and have experienced pain after staying in the sun since I was about 2 years old. When I was 2, I was outside and all of the sudden I started crying. Nobody knew why and my parents asked themselves whether or not I was pretending. Slowly they figured it had to do with the sun. We tried so many things and we went from doctor to doctor, but nobody had a clue what exactly my problem was. Several times my eyes were so swollen I couldnt see anything. In the summer it was horrible. At night I couldnt sleep, I itched myself until I was bloody awake or sleeping. The only solution for me was to protect myself and to stay out of the sun. But I didnt want to be different from my friends and I didnt want to be a burden for my family. So I often crossed the border, to make it possible for my family to take me with them.
When I was about six or seven, I met a doctor by chance, who guessed what my problem was. She sent me to a university hospital, where my family and I got a diagnosis: Erythropoietic Protoporphyria. Just this fact helped us a lot.
For a long time I thought I was the only one having this stupid problem. But then my mother found a support group for German EPP patients. We went to a meeting and it was so strange hearing people talk about things I experienced as well. My family supports me a lot but they cant understand me like someone with EPP is able to. Just simply talking with someone so similar was great. I got to know a girl about the same age as I am and we became very good friends. Last year we spent two weeks in Greece. During day we stayed inside or in the shade and in the late afternoon we lay on the beach.
Growing older I got to know my limit. Now being more responsible for myself, I have to measure the fun and the pain I likely will have when I do any outdoor activity. By now Im so self-comfortable that I dont feel strange anymore wearing my huge hat and long sleeve. I try to avoid taking pain killers, but sometimes its inevitable even though I protect myself.
EPP of course limits me in certain ways, but sometimes I dont care. Having an awesome day downhill skiing, a class trip to Rome (all day sunny, 42°C the time I was there) or having fun at a bike-tour with friends is worth having any pain.
Rememberâ?¦.. Research is the key to your cure!
FDA Letters From People with EPP
Sunday - May 5, 2013 @ 16:19:06
FDA Letters From People with EPP
EPP friends and family members of EPP people please get your pen and paper out and write a letter to the FDA. The reason is that we need to assure them that people with EPP are in grave need of a treatment.
Many health professionals and health departments have the opinion that a life style change is all that is needed for EPP. In other words, stay out of the sun and the person with EPP will be fine. People with EPP and their family members need to change their opinion, particularly since the FDA will be assessing a new treatment, Afamelanotide / SCENESSE for approval or not.
Please take a few minutes of your time to write a letter to the FDA describing your experience with EPP, how it has negatively impacted your life and how much you need a treatment for the disease. This letter will accomplish more than you can imagine. All you need to do is write the letter addressed to
Margaret Hamburg, M.D.
Commissioner, Food and Drug Administration
10903 New Hampshire Ave
Silver Spring, MD 20993-0002
*BUT DO NOT MAIL IT TO THEM*. Rather send it to the APF so we can deliver all the letters to them personally. We also ask that if a few EPP patients who are willing to speak with them in person would like to attend the meeting, as well. If you would like to participate, please contact Desiree at the APF office 1.866.APF. 3635
This is a simple but important task that will only take you minutes. You have the opportunity to have a new treatment for EPP. Our researchers have worked very hard to complete the research for FDA approval. Please honor their work with your letter.
Rememberâ?¦.. Research is the key to your cure!
Thank you,
Desiree Lyon Howe
UTMB Health Porphyria Center Research and Testing Center
Sunday - May 5, 2013 @ 16:13:56
Porphyria Research at UTMB
Our laboratory group has a longstanding interest in the human porphyrias, which are rare disorders that are due to alterations in the enzymes that synthesize heme. Our research focuses on developing new therapies and strengthening the evidence for existing therapies. We primarily design and conduct prospective studies, rather than retrospective studies of existing records, and these require significant numbers of well-characterized patients with whom we have positive ongoing relationships. Many patients with porphyria are inadequately diagnosed and managed, because there are few specialists with adequate experience. To engage large enough patients countrywide, we need to provide advice on what they need in terms of more accurate diagnosis and better treatment. Other centers have mostly emphasized nonhuman studies or molecular research that does not require prospective relationships. Engagement with the extended community of porphyria patients also highlights issues that the community thinks need further research.
In seeking to find and establish with enough patients for research, we interact frequently with patients, family members and physicians at a distance, and respond to their requests to provide advice on diagnosis and treatment. We also maintain the only laboratory in an academic institution in the US that is certified to accept samples for diagnostic biochemical testing, and we issue reports that include detailed interpretations of the results. The American Porphyria Foundation (APF) is an active and very effective patient support group that helps us engage the porphyria community and recruit patients for study. They also raise funds from members, private donors and industry for research and development work that this community thinks is important. Especially important is the APFs Protect The Future (PTF) program, which supports training of new porphyria specialists and scientists at academic institutions such as UTMB. As an APF initiative, the PTF program is an effort that is a clear example of effective community engagement.
More recently, the 5 major porphyria centers in the US and the APF formed the Porphyrias Consortium and applied successfully for a U54 grant from NIH to support collaborative clinical research and training the next generation of porphyria experts. The participating centers in addition to ours are at Mt. Sinai in NY, UAB, U of Utah and UCSF. An unfunded 6th center in Charlotte NC has been added and is engaged primarily in training. The PC is one of 19 consortia in the Rare Disease Clinical Research Network (RDCRN: http://rarediseasesnetwork.epi.usf.edu/). The RDCRN includes a Data Management and Coordinating Center (DMCC) at the University of South Florida that is supported by a separate grant, and it provides invaluable infrastructure support to the PC and other consortia for research (protocol development, web-based data entry and warehousing, statistical consultation, site monitoring, a DSMB, etc.), website development, meetings and conference calls. The PC has already initiated a longitudinal study of all the porphyrias, conducted a clinical trial sponsored by industry, and is preparing additional clinical trials and pilot studies. All investigators meet face-to-face quarterly and have monthly conference calls. Training activities have increased, and now include a training week here in Galveston, which reflects our having the greatest number of available patients. The PC website includes a Patient Registry, where patients can ask to be contacted for information about prospective studies or other needs. At its own website, the APF has developed an on-line interactive database of safe and unsafe drugs, which addresses an important clinical issue for the several acute porphyrias (http://www.porphyriafoundation.com/). APF-initiated community engagement activities also include scheduled conferences and conference calls between patients and an expert from one of the centers. We have also advocated for porphyria research and new drug development at the FDA and NIH in Washington. Therefore, the PC and RDCRN have raised porphyria clinical research and community engagement through the APF to a new level.
Youve probably got what you need. Maybe youre already in good shape, and no big health concerns. Youre having a good time, youve got a nice place to live, a job, and the problems you do have are way more important than making up any health issues which arent even getting in your way.
Doing what youre doing is easy.
But what people dont realise is caring about health can be just as easy. The hardest part, is actually change itself.
When you are enjoy the way you live, exercising the way you do and eating in a way you truly appreciate, being healthy is not hard. But learning to appreciate some of these is hard for some people, when they have done it differently their whole lives. But once you can achieve this mindset there no more trying, no more frustration. This is why I always say lifestyle is the key to long term success and diets suck. Some people take on all the principles I would recommend, but its all short-term. They havent told themselves in their mind this is the way they want to live from now on. They are usually looking for the numbers on the scale to change.
It takes mental effort, and a little perseverance to change deep ingrained habits. Why bother? Why be healthy? Youre OK now, theres nothing wrongâ?¦
Well, Im always going on about living longer, feeling better, looking better, having more energy, being mentally alert, not getting fat, or worrying about getting fat, or not getting ill so much, or recovering from illness faster.
Some people want these things, but for many, the possibility is still not enough to motivate change.
These are things its hard to go out and buy (except for drugs in some cases but Im sure you dont need educating there). These things take a long-term view. The results pay off over time. You wont eat fish today and wake up smarter tomorrow.
The sad things is, people often find the determination to change only when things get bad. You hear about people suddenly facing a life threatening illness which puts their problems in perspective, and then they realise why its worthwhile. Sometimes they make a miraculous recovery.
But smart people dont wait for threatening circumstances to motivate them, they are the people who would pursue the reward than be pushed by the pointy stick (Im sure theres a better metaphor out there). They have goals to achieve. New perspectives. Becoming better people, not just physically, but mentally too. Becoming a human being which they are proud to be.
Making the kind of changes were talking about gives you a personal power over your own life and outcomes which many people have not achieved. They accept where they are and dont move forward. But change makes life interesting. You can go your whole life doing what youre doing and getting the results you have always got. Or you can question what is possible for you, and find new ways to reach a potential you never realised existed.
Being healthy is just one way to help you reach new levels of greatness. Whatever it is you choose to be.
Remember.Research is the key to your cure!
Michele Ludewig PCT
Saturday - May 4, 2013 @ 14:27:03
Michele Ludewig
Type of Porphyria:
Porphyria Cutanea Tarda (PCT)
I was diagnosed with Porphyria Cutantea Tarda (PCT) in 1983 at age thirty seven. I had always had horrendous skin and infections of the skin. Within twenty-four hours of sunbathing, I broke out in patches of blisters on my forearms. This was the first symptom. But for a long time before this, my hair had been growing much faster than normal and my fingernails would split and crack off the top layer. My face had developed a brown racoon mask. But I didn't feel ill. These blisters intensified with more sun exposure and broke open into sores which wouldn't heal. My skin was so thin that the slightest bump would tear a piece of it off and then another sore to heal. It took over eight months to get it under control the first time. I had to get really pushy with my family doctor to get to a specialist, but when I did, he was a gem and was familiar with porphyria. God bless him. We have a list of do's and don'ts that have worked pretty well. I came out of remission two more times, the last being in 1990. I have had some other odd and unexplained illnesses and experiences and hope to get to the heart of it all as time goes by. Blessings to all of you.
Remember.Research is the key to your cure!
The Porphyrias Consortium Genetics 101: Basic Genetics and Inheritance
In order to better understand the Porphyrias and how the disorders are inherited, it is helpful to understand some concepts of basic genetics and inheritance patterns.
DNA, Chromosomes, and Genes:
Deoxyribonucleic acid (DNA) is a nucleic acid that contains the instructions used in the development and functioning of all known living organisms and some viruses. DNA is often compared to a set of blueprints or a recipe or a code because it contains the instructions needed to make certain proteins, which are the complex molecules that do most of the work in our bodies. Each of these proteins has a specific function in the cell, and, ultimately in how the organism develops, its physical makeup, and how it functions day-to-day. The DNA segments that carry this genetic information are called genes. The size of each gene varies greatly, and there are about 20,000 genes that are distributed along the 23 pairs of chromosomes.
A DNA molecule is a twisted double-strand of building blocks, called nucleotides. It is like a twisted ladder, with the vertical stringers made of phosphates and sugars and the rungs made of pairs of nucleotides. There are four nucleotides in DNA: adenine (A), thymine (T), guanine (G), and cytosine (C). Also important is that on each rung of this ladder, A always pairs with T, and G always pairs with C. These nucleotides along the ladder are like letters in a word, and put together in their specific order make up the words in a detailed set of instructions. These instructions are read using a special code, called the genetic code.
Within cells, DNA is organized into long structures called chromosomes. A chromosome is like a cookbook with many recipes (or genes) that tell the body how to function. The human body is made up of trillions of cells and over 200 different cell types like various blood, liver, and brain cell types. Each cell contains 46 chromosomes. Each chromosome can be identified by its relative size and location of the centromere, a constriction in the chromosome.
The chromosomes come in pairs. Since there are 46 chromosomes, there are 23 pairs of chromosomes. One chromosome in each pair comes from the persons father. The other chromosome in each pair comes from the mother.
The first 22 pairs of chromosomes are called autosomes. The autosomes are numbered 1-22. These chromosomes determine an indivduals physical appearance and tell the body how to function day-to-day.
The 23rd pair of chromosomes is called the sex chromosomes. Parts of these chromosomes determine whether an individual will be male or female, but they also carry additional important information. A female has two X chromosomes. A male has one X chromosome and one Y chromosome.
Along each chromosome, there are thousands of genes. Since the chromosomes come in pairs, the genes along them also come in pairs. This means that the genes that are found on one chromosome in each pair are the same as the genes that are found on the other chromosome in that pair. The sex chromosomes are an exception. Most of the genes that are located on the X chromosome are different from the genes that are located on the Y chromosome. For example, the ALAS2 gene, involved in X-linked Erythropoietic Protoporphyria (EPP), is on the X chromosome, but is NOT on the Y chromosome.
Each gene is a set of instructions that tells the cell how to make a specific product called a protein. These proteins have the job of telling the body how to grow and develop as well as how to do all the things that are necessary for the body to work properly every day. Any change in one of these genes may interfere with the bodys ability to make one of these necessary proteins. A gene change is called a mutation.
Autosomal Dominant Inheritance:
Since autosomal genes always occur in pairs, with one coming from each parent, individuals with an autosomal dominant form of porphyria [Acute Intermittent Porphyria (AIP), Hereditary Coproporphyria (HCP), Variegate Porphyria (VP), familial Porphyria Cutanea Tarda (f-PCT)] have one non-working gene with a mutation on one chromosome, paired with a working (or normal) gene on the other chromosome. Usually, the non-working gene was inherited from one of the individuals parents. Rarely, a new mutation (also called a de novo mutation) can occur in the affected individual and not be present in one of his parents. However, the de novo mutation will be inherited by 50% of the patients offspring. In individuals with an autosomal dominant form of porphyria, there is a 50% chance with each pregnancy that the non-working gene will be passed on to a child. Some of those who inherit the non-working gene will develop symptoms.
Autosomal Recessive Inheritance:
Individuals with an autosomal recessive type of porphyria [Congenital Erythropoietic Porphyria (CEP), Erythropoietic Protoporphyria (EEP) and Hepatoerythropoietic Porphyria (HEP)] have a pair of genes with mutations that affects the function of the enzyme encoded by the gene. In such individuals, one mutant gene was passed on from each of their parents. If their children only inherit one mutant gene for that porphyria, which will be paired with a normal gene from the other parent, and the child will be a carrier, but will not have symptoms.
If two carriers of the same or similar mutant recessive gene have children, there is a 25% chance with each pregnancy that the child will inherit two mutant genes (one from each carrier parent), and these children will develop symptoms of the disease.
X-Linked Inheritance:
The sex chromosomes are the X-chromosome and the Y-chromosome. Females have two X-chromosomes, and males have one X-chromosome and one Y-chromosome. In X-linked disorders [for example, X-Linked Protoporphyria (XLP], the gene is located on the X-chromosome, and the risk for children depends on the gender of the affected parent. If a female has the mutation, there is a 50% risk for passing the mutation onto her children with each pregnancy.
X-linked inheritance (when the mother has the mutation)
If a daughter gets the gene mutation from either her mother or her father, the daughter may or may not have symptoms, and the severity of symptoms may vary even among the females in the same family. For this reason, in most X-linked disorders, including X-Linked Protoporphyria, females who have the gene mutation are referred to as heterozygous for the mutation, rather than carriers which infers that they will not have any symptoms (as in autosomal recessive disorders). If a son gets the mothers mutation, he will have symptoms.
Remember..Research is the key to your cure!
Clinical Studies
Saturday - May 4, 2013 @ 14:16:00
Clinical Studies
There are two main types of clinical studies: clinical trials and observational studies. In a clinical trial, there is some form of treatment intervention. There is no intervention in an observational study, which is aimed at observing patients to better understand the long-term course of their disease. Clinical trials are used to test new treatments before they are approved for use by the FDA. This type of trial gives patients a chance to try out a new medication in its early stages. As with any experiment, the result of a trial is not known before its conclusion. Your participation could help demonstrate a terrific treatment breakthrough, or it could help scientists discover that a new treatment does not work after all. There may be some risk involved from the treatment in a clinical trial. Participating in either a clinical trial or an observational study is a serious responsibility. Volunteering to participate could be a way to help yourself, affected family members and other patients by advancing medical and scientific knowledge of your condition. Some patients derive great satisfaction from assisting doctors in the study of their disease. Participation in a study can also mean a chance to meet a porphyria researcher in a clinical setting, and the consultation can be beneficial. For information on porphyria trials currently recruiting patients, call the APF office or visit NIHs clinical trials website: Clinical Trials of Medical Treatments: Why Volunteer? might also be useful reading as you think about whether youd like to participate or not.
Remember..Research is the key to your cure!
CEP~ What is it?
Friday - May 3, 2013 @ 18:28:35
Congenital Erythropoietic Porphyria (CEP)
This disease is extremely rare and is autosomal recessive. It is also known as Gunther's disease. The deficient enzyme is uroporphyrinogen III cosynthase (or uroporphyrinogen III synthase). Various mutations in the gene for this enzyme have been identified in different families. As is characteristic of the erythropoietic porphyrias, symptoms begin during infancy. Sometimes CEP is recognized as a cause of anemia in a fetus before birth. In less severe cases symptoms may begin during adult life. Porphyrins are markedly increased in bone marrow, red blood cells, plasma, urine and feces. Porphyrins are also deposited in the teeth and bones.
Symptoms
Skin photosensitivity may be extreme, and can lead to blistering, severe scarring and increased hair growth. Bacteria may infect the damaged skin. Facial features and fingers may be lost through phototoxic damage as well as infection. Red blood cells have a shortened life-span, and anemia often results. Synthesis of heme and hemoglobin are actually increased to compensate for the shortened red blood cell survival.
Treatment and Prognosis
Blood transfusions and perhaps removing the spleen may reduce porphyrin production by the bone marrow. Activated charcoal given by mouth is sometimes effective. Bone Marrow Transplantation has been very effective in some patients. Stem cell transplantation and gene therapy may also be an option in the future.
Remember..Research is the key to your cure!
APF Volunteers come together to raise Porphyria Awareness
Wednesday - May 1, 2013 @ 19:04:19
We want to send a big thank you to our longtime APF member and longstanding volunteer, Amy Chapman.
Amy Chapman, who has AIP, has been a major force for the APF. She has been a volunteer Administrator on our APF Facebook support groups since their inception and in that capacity reaches out to each of the 1,000 plus members. Amy has graciously shared her experiences, and knowledge of valuable resources provided by the APF. Amy also writes the APF Purple Light blog.
Amy has shared her AIP story on a video for national media. You can view Amy's video on the APF YouTube channel: PorphyriaFoundation
For this year's National Porphyria Awareness Week, Amy Purchased items to sale to raise money and awareness for Porphyria. Many of the items have the APF logo on them and 100% of the profits went to the APF to advance Physician Education. Orders still can be placed through May 6, 2013. To view these items and learn how to order go to: Amy's Fundraising Event.
Thank you to all of our APF volunteers who did an amazing job of raising porphyria awareness from placing Awareness Week posters on their Facebook pages to hosting Health Fairs and more. Watch the APF Enews for the next wonderful story about the young Cook brothers and their family efforts to enhance porphyria awareness with their HAT DAY event.
Remember..Research is the key to your cure!
Remember.Research is the key to your cure!
Wednesday - May 1, 2013 @ 18:42:19
Remember.Research is the key to your cure!
Take a walk with me a poem for Porphyria Awareness Week by Victoria Harrold
Take a walk with me Spring is coming Excitement fills the air Jumpers replaced by short sleeves and floaty skirts. Who is to get the better tan? Not me, thats for sure For I live in the shadows. I long to wear short sleeves and bright, floaty, short skirts But for me I have to cover head to toe. For me the sun hurts. Clouds are so amazing Each with their different shapes and details They even have names like Cirrus or Stratus For me these clouds offer safety From the suns harmful rays. Oh how I long to be sat for hours In a daze, enjoying the warmth That the sun shares with so many. I have EPP So that cannot be Hopping from shadow to shadow. Which pair of gloves shall I wear today? Does that hat go with that long skirt? What if someone notices me And mocks me For I dont dress the way they do. People struggle to understand a disease you often cannot see The pain is so intense More than anything you could imagine Independence gone Oh please stop For I cannot take what you do For why you hurt me so People try to capture it By saying things like Oh I have hives Or Its just like sunburn. This is not sunburn! This is not hives! This is my body crying Whats happening? Why do I burn? Off indoors I must go Watching everyone else People looking at me in strange ways For they cannot understand. I want to go out today But what does the weather say? A bright and sunny day we shall have Oh no, here we go again. Alone I often feel But now I know of those who suffer just as I do Pain, swelling, blistering, hallucinations Yes, we know pain For this is not your average sunburn. Modern lights are the way forward They are amazing They save so much in electric. For me with EPP These lights make me sick For they are just like the sun So bright So painful. Shopping now a chore For Im not sure Of what is above my head Until my face feels the burn And I know that here we go again Leave! Leave! Leave! Vampires suck for we have the same branding as them We have EPP We cannot absorb as much iron as others Our body rejects it So we are pale And tired. Genetics we are A lab study. Faith has kept me strong In the hours of my pain I am given hope That my God is with me Im not alone He understands He doesnt question my sanity He keeps me going For I have EPP Take a walk with me.
Members Request Recap or items to sell for APF Fundraiser!
Tuesday - April 30, 2013 @ 15:47:19
5:00pm 5/1/13 UPDATE~ Ok here is a recap per members request on what is left to sell. All orders need to be placed by May 6th. Only by a money order or personal check to Amy Chapman. To place your order you MUST EMAIL to: porphyriaorders@gmail.com If your order has two large items or more, {I will let you know shipping costs) it includes materials, tracking and postage. So here are the items/left.
1.} 16 gig USB Drive apf logo 15.00 each {7 left} 2.} Women's Scarf- 1 hot pink & 1 pretty peach 7.99 each 3.} Apf Logo Tote Bag and Water Bottle- 10.00 each {4 Black) Red/Blue/Purple APF logo 4.} Double Wall Travel Mugs with Flip Top Lids APF/gifts inside 9.99 each (2 Orange left) 5.} Dog Toys with Squeaker- 4.50 each 6.} Kitty pillows fresh natural catnip 4/10.00 or 2.50 each 7.} APF~ Porphyria wristbands 2/6.00 dark blue, red, light blue 8.} Women's Sun hats 2 Brown 1 Tan 15.99 each 9.} Men's/Women's Fedora Hats with Trim 10.99 each 2 Tan, 3 Red, 2 Brown 10.} Re-useable Totes 2 Blue/White 1 Black/White with Logo 5.99 each I am NOT taking orders from FB.
Monica Fleegels Fundraising / FDA letter writing / Porphyria Awareness Campaign.
Wednesday - May 1, 2013 @ 18:45:09
Monica Fleegels Fundraising / FDA letter writing / Porphyria Awareness Campaign.
"Last summer, due to the tireless efforts of the APF , I was able to participate in Phase III clinical trials that gave me relief from the pain of EPP (Erythropoietic Protoporphyria). For the first time in my life , I spent time in the sun with my family and friends!! The APF was able to convince the FDA of the importance of continuing the trials and now we need to inform the FDA that they need to approve Scenesse , so all who suffer from EPP can spend time in the sun. Through a letter writing campaign and your donations, we can assist the APF with this major endeavor." Monica Fleegel
Monica developed a very creative idea to raise Porphyria Awareness, as well as a means to fund the APF Physician Education program and acquire letters from family and friends to advise the FDA about the importance and need for treatment for EPP. Monica prepared a fundraising event on the APF - FirstGiving fundraising website. Plus, she hosted a fun event to gather her friends and family together to write letters to the FDA about how EPP has affected the Fleegel family.
Monica reported, "So far $2,270.00 has been raised, about 20 letters and 50 people showed up to the fundraiser. It was very successful! People were so generous."
We sincerely thank Monica and all of her generous family and friends who participated in this wonderful event. The members of the Fleegel family with EPP have been very active with the APF, even participating in a documentary on the subject shown in Europe.
Cookie made by Monica's Daughter.
National Porphyria Awareness week is held once a year. It is up to us all to continue Porphyria Awareness every chance we get. The APF has some great materials that you can carry with you when you visit your Doctor, or the Emergency room or any other contact you have with the medical community.
If you would like some of the Porphyria educational supplies, please contact the APF office: 1.866.APF.3635 and request them today.
Remember..Research is the key to your cure!
RareConnect announces 40th online community
Monday - April 29, 2013 @ 20:08:02
RareConnect announces 40th online community
RareConnect.org, the platform created, monitored and run by patient organisations EURORDIS and NORD, continues its mission of bringing rare disease patients together, across borders and beyond language barriers
Paris, 30 April, 2013 RareConnect.org, a flourishing rare disease online network that brings together thousands of frequently isolated patients, families and patient groups, from across the globe, celebrates the launch of its 40th community. Each of RareConnects disease specific communities is monitored, offering a safe place for exchange. Information and comments are translated into five languages, allowing users to communicate with each other despite language differences.
This 40th RareConnect community offers those caring for patients with rare undiagnosed brain diseases a place to come together and connect. The community was created in collaboration with several patient support groups including the Wilhelm Foundation,SWAN UK, and SWAN USA.
Commenting on the launch of the new community, Wilhelm Foundation founder Helene Cederroth said, This community represents an enormous step forward to better understanding undiagnosed brain diseases. It is a big opportunity for the community to make its voice heard and hopefully it will encourage specialists from all over the world to participate so that one day we hope it can lead to diagnoses.
RareConnect launched in 2009 as part of the strategic partnership between the worlds two most established rare disease patient organisations, EURORDIS (European Organisation for Rare Diseases) and NORD (National Organization for Rare Disorders). The platform provides a safe, moderated online social network where individuals affected by rare diseases can connect with others, share common experiences and find helpful information and resources.
Organised into 40 disease specific communities, the network now counts more than 4,300 members and involves over 300 patient associations in the governance and growth of the 40 communities. Three full-time community managers support the moderators, animate and promote the project. Volunteer moderators from many of the member groups take an active role in their respective communities.
Available in five languages (English, French, German, Italian and Spanish) RareConnect is unique in that it offers a human translation service to patients who need to exchange valued experiences and information with members from different countries, speaking different languages. This service available free-of-charge allows discussions, articles and patient stories to be shared and understood across the five main European languages, permitting people to learn how others are coping with their rare diseases in different countries.
EURORDIS Chief Executive Officer Yann Le Cam said, RareConnect brings together rare disease patients in a collaborative way, across borders. Its rapid success is beyond our expectations. Watching it expand and taken to the hearts of hundreds of patient groups as a safe place they can call their own is our inspiration.
RareConnect stands apart from other rare disease networks by not carrying advertising or sharing data with any third parties. It hosts thriving communities that include rare conditions such as Dravet syndrome, Multiple System Atrophy, and Behcet's disease. Visit the RareConnect website for a full list of the current rare disease communities.
RareConnect project leader at EURORDIS, Denis Costello, said, We developed RareConnect in response to the need of rare disease patients to connect with each other and to have access to reliable information from trusted sources. Patients - or those caring for them - frequently find it difficult or impossible to obtain a diagnosis, or to access relevant information. Often there is a lack of medical expertise where they live. RareConnect helps patients and families to find what they need, including information they can take back to their own doctors.
For more information or to speak to EURORDIS RareConnect Project Leader Denis Costello, please email denis.costello@eurordis.org or call +34 6 71 88 22 18. Patients or patient organisations interested in partnering with EURORDIS or NORD to develop an online community for their rare disease, can contact: robert.pleticha@eurordis.org
Rare diseases are life-threatening or chronically debilitating diseases. Due to the low prevalence of each disease, medical expertise is rare, knowledge is scarce, care offering inadequate, and research limited. Very few cures exist. While each disease is rare, collectively they affect more than 60 million people in Europe and the USA alone. Despite their great overall number, rare disease patients are the orphans of health systems, often denied diagnosis, treatment and the benefits of research.
The European Union considers a disease as rare when it affects fewer than 1 in 2,000 citizens. Approximately 80% of rare diseases have a genetic origin. Over 6000 different rare diseases have been identified to date, affecting an estimated 30 million Europeans collectively.
About EURORDIS
EURORDIS is a non-governmental patient-driven alliance of patient organisations representing 571 rare disease patient organisations in 52 countries. We are the voice of 30 million people affected by rare diseases throughout Europe.
Further details concerning EURORDIS and rare diseases are available at:www.eurordis.org
About NORD
NORD is a non-profit organisation representing all individuals and families affected by rare diseases in the USA. It was established in 1983 by patient organisation leaders who had worked together to get the Orphan Drug Act adopted. NORD provides programmes of education, advocacy, research and patient/family services to improve the lives of Americans affected by rare diseases. Learn more about NORD at www.rarediseases.org
Press Contact
Denis Costello
EURORDIS Web Communications Senior Manager & RareConnect Leader
Please show your support and don't forget: The last day to place an order for the APF Awareness will be May 6th. If you plan to make a purchase remember 100% of your funds go directly to the APF. For ordering questions/placing an order email me American Porphyria Foundationporphyriaorders@gmail.com Remember~ Research is your key to a cure!
SCENESSE~ What is it and how does it help Porphyria Patients
Friday - April 26, 2013 @ 18:22:17
SCENESSE (INN: afamelanotide) is Clinuvel's proprietary first-in-class photoprotective drug. Clinuvel has submitted a marketing authorisation application (MAA) for SCENESSE to the European Medicines Agency for the orphan diseaseerythropoietic protoporphyria (EPP). Further studies of SCENESSE are underway as a repigmentary agent in vitiligo and as a photoprotective for organ transplant recipient (OTR) patients.
SCENESSE (pronounced "sen-esse") acts by increasing the levels of melanin in the skin; and shields against UV radiation (UVR) and sunlight. SCENESSE is delivered via a subcutaneous dissolving implant approximately the size of a grain of rice. Increased pigmentation of the skin appears after two days and lasts up to two months.
Alpha-Melanocyte Stimulating Hormone (α-MSH) is a naturally occurring peptide hormone which is released by skin cells in response to the stimulation by ultraviolet radiation (UVR). α-MSH has a very short half life (seconds) in the blood stream, sufficient to reach and stimulate other skin cells (melanocytes) which in turn produce and release melanin, a dark brown pigment. Melanin is known for its photoprotective effect.
The skin's response to damage from UV radiation - Human tanning response
SCENESSE is a chemical analogue of α-MSH and is a linear peptide with 13 amino acids. Two amino acids present in α-MSH have been changed and amplified to produce afamelanotide. This small change creates a more stable molecule with increased potent biologic effects and a longer half life (minutes). SCENESSE increases melanin content of the skin without exposure of the skin to the damaging effects of UVR.
Clinuvel is currently trialing SCENESSE in a range of light and UV related skin disorders (photodermatoses) and as a repigmentation therapy in vitiligo. It is proposed that SCENESSE will provide prophylactic treatment to patients suffering from photodermatoses by stimulating melanin to act as a photoprotective filtering the impact of UV to the skin. In vitiligo the drug is being evaluated in combination with narrowband ultraviolet B phototherapy (NB-UVB).
Over 700 patients have been treated with SCENESSE in more than 20 clinical trials over several indications. Results to date suggest that the drug is well tolerated. In EPP trials, SCENESSE has been shown to reduce the incidence and severity of phototoxic reactions.
Biomimicry of the human tanning response
Clinuvel Pharmaceuticals Ltd is an ethical pharmaceutical company focused on providing photoprotective care of the skin. Clinuvel is working closely with global regulatory agencies to develop SCENESSE as a prescriptive drug. Clinuvel has been developing and testing SCENESSE since 2000. Our development is focused on the SAFE and controlled administration of the drug substance.
WE STILL NEED YOUR PERSONAL LETTERS ON HOW THESE DRUG HAS HELPED YOU! TIME IS RUNNING OUT. CONTACT THE APF 866-APF-3635 FOR MORE DETAILS. WE NEED THIS DRUG APPROVED.
Remember..Research is the key to your cure!
Student Educates Classmates during National Porphyria Awareness Week
Wednesday - May 1, 2013 @ 18:47:36
Thank you to all who participated in the National Porphyria Awareness week.
We would like to sincerely thank everyone that was involved in last weeks National Porphyria Awareness activities.
The following is an example of one of the Campaigns one of our young EPP members Alessia Callahan does every year for Porphyria Awareness Week. We are so very proud of her.
Student Educates Classmates during National Porphyria Awareness Week
Thomas E. Bowe student Alessia Callahan speaks to her fifth-grade class about Erythropoietic Protoporphyria during National Porphyria Awareness week.
GLASSBORO - Alessia Callahan faces challenges that other 11-year olds don't even have to think about. While those challenges make her unique, her courage in facing them makes her extraordinary. Read the full article here.
Stay tuned. We will be sharing more Porphyria Awareness campaign experiences with you in the near future.
Remember.Research is the key to your cure!
Sign UP its free, Lifesaving. Porphyria Invite.
Friday - April 26, 2013 @ 12:37:29
I wanted to take a few moments to suggest signing up for these groups. These groups are designed for you at no cost.
When you sign up for the http://rarediseasesnetwork.epi.usf.edu/porphyrias/index.htmyou are signing up to participate in research projects answering questions about your type of Porphyria, you have questions, your chance to support these programs for possible medications and cures are so necessary. These are great Expert Doctors that are interested in learning about you and your family. Sometimes its a simple process of answering questions, a phone call, a trial drug, or a blood & urine sample! So please sign up and explore this site.
Next we have the http://porphyriafoundation.blogspot.com. This is supported by the American Porphyria Foundation. It is also free to join. Learn about upcoming events, read members stories, be encouraged that you are not alone. Try a recipe, learn some tips from the Experts. Be INVOLVED!
Do you enjoy interacting with other patients, doctors from all over the world that also have Porphyria? I know I do. When you sign up for free to a program called: RareConnect~https://www.rareconnect.org/en you can find diagnosed Patients with all types of people all over the world, new and exciting news, learning opportunities, announcements, how medicine and trials are making progress, start discussions get answers. Learn how Porphyria affects each one of us.
So what are you waiting for, please join your support, experiences and encouragement are what we all need. Please show your support for such programs they may not always be available to us.
Remember..Research is the key to your cure!
Read Kelly Story & PCT
Thursday - April 25, 2013 @ 15:02:40
Kelly Story
Type of Porphyria:
Porphyria Cutanea Tarda (PCT)
My name is Kelly Story and I live with my husband, Chad, and two cats in Kissimmee, FL. In July of 1999, one month after our wedding, I was out of town on business, and I noticed tiny little water blisters all over my hands. The blisters didn't itch and were not painful. Although I found them to be very odd, I didn't worry much.
Over a short period of time, my skin became extremely fragile. It seemed like almost anything would cause a scrape on the skin of my hands. Plus, the blisters got much worse. My hands looked like something out of a horror movie. I was so embarrassed all of the time, and I cried a lot. I went to a dermatologist. After two visits, he told me that he was fairly certain that I had PCT but suggested that I go to a specialist. After several humbling tests and weeks of waiting, I was officially diagnosed with PCT.
The doctor said that I would have to start phlebotomies. This meant that over a pint of blood would be taken from me at one time. Even after I began the phlebotomy treatments, the blisters moved to my arms. These blisters itched tremendously. My poor husband didn't know what was happening, because, I would wake up in the middle of the night with a frenzy of scratching and crying. The itching was unbearable. I would feel so guilty afterwards. After all, I was receiving treatment for my condition and knew that I did not have a fatal disease. There are other people in the world with so much more serious problems. But, it was still uncomfortable, and my hands and arms were just so ugly.
I was tired a lot during the six month or so period I was having the phlebotomies. The doctor said that I would most likely be temporarily anemic. This was the result of having the blood taken from me. I used to do aerobic exercises at least four times a week, but that stopped. I also got headaches quite often. Finally, I was in remission. No more cuts, no more blisters, and no more itching.
I lived for a while with the dark scars on my hands from all of the sores and blisters and several lighter ones on my arms. But now, the scars have faded tremendously. You can't see any on my arms, and the ones on my hands are very pale. It may sound vain, but I never thought I would have pretty hands again, and now I do. To this day, I still cringe if I accidentally knock my hand into something. But, I am always relieved when I look down and see no scrape or cut.
Since being diagnosed with PCT, I've taken estrogen and alcohol out of my life, and I try my best to stay out of the sun. It's hard living in Florida, but I just keep applying that good old sunscreen. I'm very blessed to have such a supportive husband. I told Chad on our first date that I was high maintenance. Boy, neither one of us knew how much!
Remember~ Research is your key to a cure!
What Real Happiness Is All About? How Do We Get It?
Wednesday - April 24, 2013 @ 20:37:24
When you SEEK HAPPINESS for yourself, it will always elude you. When you seek happiness for OTHERS, you will find it yourself. ~ Wayne Dyer
What is it that motivates you in life? What are the things you THINK are making you happy, and what are the things that really make you happy? Are you able to observe yourself from time to time and see whether the things you chase after are really the things you want for yourself?
I think that most of us, want to want more than they want to have, because when they receive that which they were after, they go on to the next thing, and the next thing, and this is how most of us spend our lives, running after something that we think it is outside ourselves, believing that our happiness lies in things, in other people, in different places, etc., and we rarely or never, stop to observe ourselves and our behavior, we rarely or never stop to think whether we are sane or insane for doing so.
It is never too late to return to yourself, never. I challenge you to do this. I challenge you to start observing your thoughts, your desires, your feelings and behaviors, I challenge you to become the observer of your own live, and believe me, by doing so, you will discover so many new and incredible things about yourself, you will find out so many things about your real powers, about the meaning of life, and about the meaning of real happiness.
From my own experience, I will have to tell you that, whenever I see happiness as a selfish act, when I think that by going to a certain place, having a certain thing, etc. I will be happy, almost 100% of the time I am wrong. What I have discover over the years, after doing so much introspection and observing myself and the many people around me, is that happiness is not a place you go to, happiness is not a person, happiness is not a dream you achieve, happiness just is. Is this simple.
We will find happiness the moment we stop to see the self as self, the moment we start to see ourselves as being one with the whole world. No matter where you are and no matter what you do, no matter how you look and no matter how much or less you have, etc., if you are not happy in that specific situation, if you are not happy with what you have and with who you are, you will not be happy if you change the environment., if you change your looks, your job, your partner and your friends. You may delude yourself into thinking otherwise, but in the end, you will go back to feeling the way you do in this exact moment, and you will discover that happiness is not outside yourself.
We dont want to accept this because if we do, we will have to wake up and take responsibility for how we feel, for our actions and behaviors, we will have to take responsibility for our own lives, and it can be somehow challenging to do so. For those people who are in this journey of self discovery and self mastery, as time goes by, as they will travel farther and farther away, they will discover what happiness is all about, and what really makes their heart sing, what really makes them glow, and they will discover that it is not money, it is not big houses and shinny cars, but rather having a meaning, a purpose in life, larger than themselves, larger than life.
It is always about giving, about sharing whats best about ourselves with others, because, when we do so, we travel to the most incredible places, we feel like we never felt before, and if somebody asks us to describe these states of beings, to put them into words, it will be impossible, because it is beyond that, it is beyond words.
Happiness is and will always be present within ourselves, and will come to surface the moment we decide to be true to ourselves, the moment we no longer think in tearms of ME, I, MINE, but rather in tearms of US and WE, knowing that we are all one, and that we are all together in this journey called life.
Happiness will not, and can not be found as long as we see ourselves as being separate from everybody else, as being better and more special than everybody else, this is not what happiness is. Real happiness is about sharing, about giving, the best we got to those around us, and when we do so, we will inspire others to do the same, and this is how the whole world will be transformed; this will be the moment we will realize that if we want the world to be a happy place to live, will first have to be happy ourselves, and by doings so, the whole world will be transformed.
Sooner or later, we will all discover this truth, it will all become very clear to us, and we will start to see things as they really are, not as we are
Remember~Research is your key to a cure!
Please take a moment to donate and raise awareness for The American Porphyria Foundation
Wednesday - April 24, 2013 @ 14:25:55
AMERICAN PORPHYRIA FOUNDATION~ if you are looking to still place an order with 100% of all orders going to the APF please let me know. All orders are on their way to those that have purchased things. Things that are available are the 16 gig usb drive, bag's and totes and wristbands in navy, red, purple light blue, scarfs beautiful most all colors, and traveling cups. So please email me with any questions or to reserve items @ porphyriaorders@gmail.com
Please take a moment to donate and raise awareness for
The American Porphyria Foundation
"Get Informed. Get Involved. Help FDA Help Patients Have a Bigger Voice.
Tuesday - April 23, 2013 @ 20:27:24
FDA opens new line of communication with patients
"Get Informed. Get Involved. Help FDA Help Patients Have a Bigger Voice. That's the slogan of a new FDA web site. The FDA Patient Network has been designed from the ground up to focus entirely on patients.
The FDA Patient Network web site is an interactive tool for educating patients, patient advocates, and consumers on how their medications - both prescription and over-the-counter -and medical devices move from the realm of idea to the realm of the marketplace. It brings together, in one place, information that is important to patients, making it easier for them to find what they are looking for and to understand the significance of their findings.
This web site will open new channels of communication with the public, such as live chats with senior agency officials. It will help patients and consumers better understand the process for determining whether medical products are safe and effective and encourage them to contribute their ideas and concerns about the development and regulation of these products".
This is your opportunity to let your voice be heard, and to educate yourself.
Whether youre a vegetarian, foodie, health-conscious mom, busy professional, or anything in between, there is a colorful, delicious salad just for you. If you havent found that perfect salad that you just love, youre in the right place, because we are here to help you with our completely custom, foolproof salad how-to. Just pick what you like, pile on the nutritious ingredients, and enjoy a hearty, healthy, homemade saladâ?¦
Get Inspired Now that you are armed with all the elements to create salad perfection, youll need a little inspiration, no? Here are some of our favorite saladsâ?¦
â?¢ The Busy Lady For the woman on-the-go an energy boosting lunch is a must. Power up with super foods like chicken, spinach, avocado, and goat cheese. The super charged ingredients in Recipe Girls salad will support you through your hectic schedule.
â?¢ For the Kiddos Get the kids excited about veggies with this Taco Salad Bowl from Cherry on my Sundae. This salad tastes like Mexican night, but with the health benefits of avocado,black beans, grilled chicken, and crunchy chopped veggies. Added perk? Moms and dads seem to enjoy this one, tooâ?¦
â?¢ The Adventurer Ready to step out of the box? Iowa Girl Eats mixed the unexpected flavors of apples, salmon, beets, cranberries and many more yummy ingredients to create a uniquely delicious and super nutritious lunch.
â?¢ The Veggie Lover Super delicious and packed with protein-filled lentils, this salad from the Kitchen Confidante is hearty enough to keep vegetarians feeling full and satisfied.
â?¢ You can grab more salad inspiration on our Pinterest board.
What does your perfect salad look like? Combine the ingredients above (or other favorites) and share your signature salad with us!
Remember~ Research is your key to a cure!
Learning about Porphyria, types, treatment, testing the APF partners with the NIH
The porphyrias are a group of different diseases, each caused by a specific abnormality in the heme production process. Heme is a chemical compound that contains iron and gives blood its red color. The essential functions of heme depend on its ability to bind oxygen. Heme is incorporated into hemoglobin, a protein that enables red blood cells to carry oxygen from the lungs to all parts of the body. Heme also plays a role in the liver where it assists in breaking down chemicals (including some drugs and hormones) so that they are easily removed from the body.
Heme is produced in the bone marrow and liver through a complex process controlled by eight different enzymes. As this production process of heme progresses, several different intermediate compounds (heme precursors) are created and modified. If one of the essential enzymes in heme production is deficient, certain precursors may accumulate in tissues (especially in the bone marrow or liver), appear in excess in the blood, and get excreted in the urine or stool. The specific precursors that accumulate depend on which enzyme is deficient. Porphyria results in a deficiency or inactivity of a specific enzyme in the heme production process, with resulting accumulation of heme precursors.
The signs and symptoms of porphyria vary among types. Some types of porphyria (called cutaneous porphyria) cause the skin to become overly sensitive to sunlight. Areas of the skin exposed to the sun develop redness, blistering and often scarring.
The symptoms of other types of porphyria (called acute porphyrias) affect the nervous system. These symptoms include chest an abdominal pain, emotional and mental disorders, seizures and muscle weakness. These symptoms often appear quickly and last from days to weeks. Some porphyrias have a combination of acute symptoms and symptoms that affect the skin.
Environmental factors can trigger the signs and symptoms of porphyria. These include:
Porphyria is diagnosed through blood, urine, and stool tests, especially at or near the time of symptoms. Diagnosis may be difficult because the range of symptoms is common to many disorders and interpretation of the tests may be complex. A large number of tests are available, however, but results among laboratories are not always reliable.
Each form of porphyria is treated differently. Treatment may involve treating with heme, giving medicines to relieve the symptoms, or drawing blood. People who have severe attacks may need to be hospitalized.
Most of the porphyrias are inherited conditions. The genes for all the enzymes in the heme pathway have been identified. Some forms of porphyria result from inheriting one altered gene from one parent (autosomal dominant). Other forms result from inheriting two altered genes, one from each parent (autosomal recessive). Each type of porphyria carries a different risk that individuals in an affected family will have the disease or transmit it to their children.
Porphyria cutanea tarda (PCT) is a type of porphyria that is most often not inherited. Eighty percent of individuals with PCT have an acquired disease that becomes active when factors such as iron, alcohol, hepatitis C virus (HCV), HIV, estrogens (such as those used in oral contraceptives and prostate cancer treatment), and possibly smoking, combine to cause an enzyme deficiency in the liver. Hemochromatosis, an iron overload disorder, can also predispose individuals to PCT. Twenty percent of individuals with PCT have an inherited form of the disease. Many individuals with the inherited form of PCT never develop symptoms.
If you or someone you know has porphyria, we recommend that you contact a genetics clinic to discuss this information with a genetics professional. To find a genetics clinic near you, contact your primary doctor for a referral.
Porphyria can be triggered by drugs (barbiturates, tranquilizers, birth control pills, sedatives), chemicals, fasting, smoking, drinking alcohol, infections, emotional and physical stress, menstrual hormones, and exposure to the sun. Attacks of porphyria can develop over hours or days and last for days or weeks.
The porphyrias have several different classification systems. The most accurate classification is by the specific enzyme deficiency. Another classification system distinguishes porphyrias that cause neurologic symptoms (acute porphyrias) from those that cause photosensitivity (cutaneous porphyrias). A third classification system is based on whether the excess precursors originate primarily in the liver (hepatic porphyrias) or primarily in the bone marrow (erythropoietic porphyrias). Some porphyrias are classified as more than one of these categories.
The cutaneous porphyrias affect the skin. People with cutaneous porphyria develop blisters, itching, and swelling of their skin when it is exposed to sunlight. The cutaneous porphyrias include the following types:
Also called congenital porphyria. This is a rare disorder that mainly affects the skin. It results from low levels of the enzyme responsible for the fourth step in heme production. It is inherited in an autosomal recessive pattern.
An uncommon disorder that mainly affects the skin. It results from reduced levels of the enzyme responsible for the eighth and final step in heme production. The inheritance of this condition is not fully understood. Most cases are probably inherited in an autosomal dominant pattern, however, it shows autosomal recessive inheritance in a small number of families.
A rare disorder that mainly affects the skin. It results from very low levels of the enzyme responsible for the fifth step in heme production. It is inherited in an autosomal recessive pattern.
A rare disorder that can have symptoms of acute porphyria and symptoms that affect the skin. It results from low levels of the enzyme responsible for the sixth step in heme production. It is inherited in an autosomal dominant pattern.
The most common type of porphyria. It occurs in an estimated 1 in 25,000 people, including both inherited and sporadic (noninherited) cases. An estimated 80 percent of porphyria cutanea tarda cases are sporadic. It results from low levels of the enzyme responsible for the fifth step in heme production. When this condition is inherited, it occurs in an autosomal dominant pattern.
A disorder that can have symptoms of acute porphyria and symptoms that affect the skin. It results from low levels of the enzyme responsible for the seventh step in heme production. It is inherited in an autosomal dominant pattern.
The acute porphyrias affect the nervous system. Symptoms of acute porphyria include pain in the chest, abdomen, limbs, or back; muscle numbness, tingling, paralysis, or cramping; vomiting; constipation; and personality changes or mental disorders. These symptoms appear intermittently. The acute porphyrias include the following types:
This is probably the most common porphyria with acute (severe but usually not long-lasting) symptoms. It results from low levels of the enzyme responsible for the third step in heme production. It is inherited in an autosomal dominant pattern.
A very rare disorder that results from low levels of the enzyme responsible for the second step in heme production. It is inherited in an autosomal recessive pattern.
Awareness Week What did you do to help spread the word?
Thursday - April 18, 2013 @ 16:58:37
So how did you do with raising Awareness for porphyria last week? Your comments are welcome to encourage others to support, share and discuss!
Did you tell your Doctors?
Did you let friends know?
Were you able to share how it affects you personally?
What about family do they know about the condition?
Do you know where to get correct information?
www.porphyriafoundation.com
Learn about all the types, side effects, treatments available and so much more.
Remember~ Research is your key to a cure!
UPDATED INFO FOR ORDERING PRODUCTS APF AWARENESS WEEK
Tuesday - April 16, 2013 @ 16:29:28
UPDATED INFORMATION ON ORDERING #2
Hi APF Friends and family. Order for Awareness Week has begun. Please know that you are ordering these products and 100% of the profits go to the APF. I have ordered many products these are all excellent quality items that are from retail stores. This year we will be using first giving sight and the use of my email. I am asking that each order placed please add an additional 5.00$ to cover the cost of shipping. To place an order follow these steps: Limit for shipping is 2 items for each order for hats and totes and bags.
{1.} You can place your order by sending a money order or personal check to the following address. Amy Chapman 10475 Gandy BLVD N Unit 3417 St. Petersburg FL 33702. No tax is taken and will receive a paid receipt. Suggested method per APF!
{2.} Next please send me an email {porphyriaorders@gmail.com} with Item numbers you want 1-13 and quantity (color of bag or hat) once I receive your donation I will mail all orders out. You MUST INCLUDE YOUR NAME AND FULL MAILING ADDRESS.**If out of the USA please contact before placing an order shipping rates may change**
{3.} I will email you when item is shipped. I will NOT take any orders from FACEBOOK.
I have bought these items myself and out-of-pocket. We need to keep the APF going for PTF, Supplies, Dr. Education your donations are so much appreciated. Thank you all for your support and have fun shopping.
***All Cups have Pens, APF materials, Post it notes and much more in each***
1. Double-Wall Travel Mugs with Flip-Top Lids, 16 oz.
Save money and the environment with this chic reusable travel mug! Double-wall design helps keep drinks warm or cold and the textured non-slip sleeve helps you keep a grip on hot beverages without the burn. Plus, the screw-on lid with a flip open cap helps prevent leaks and spills. Assorted among the colors shown. BPA Free
9.99 each
2. Double-Wall Plastic Travel Mugs, 16 oz.
Take beverages on the go with this convenient travel mug! Double-wall design keeps drinks hot or cold, plus cap screws on tightly and has a sliding sip opening for less spills-assorted colors. BPA Free
8.00 each
3.Kids Water Bottle
13.5 oz. With Snack holder at Bottom just twist. Wear over the shoulder strap. Assorted Colors BPA Free
7.00 each
4 Ladies Fashion Sun Hats
Hit the beach this summer in style! Or hop in the shade! Fashion sun hats are a great way to protect your skin and eyes while having fun in the sun. Great for the beach, lounging round the pool, or working in the yard or garden. 15" Ladies Fashion Sun hats, assorted between brown and tan with tan and black trim. 16.00 each
5. Fedora Hats By Burnaby of NY
Fashion sun hats are a great way to protect your skin and eyes while having fun Mens or Womans assorted between brown and tan. 10.00 each
6. Red Fedora Hats
These are daring sharp hats for a fun event or day on the town. Quality constructed. Has a black trim make's a statement. Red for the APF! Mens or Womens 19.00 each
7. Reusable Totes
A Brand you can Trust. Go GREEN! 12inW x14inH x8.5inD Prefect for meds, paperwork, lunches, Doctors Office, and comes in Black and White Floral and Turquoise Blue Both with the APF logo. 6.00 each
8. Zippered APF Bag
Zipped Bag with pockets inside and out. Comes with a Water Bottle (Black or White) Comes with APF Info, Comes in Red, Black and Green colors. This item has handles and great for overnight trips, day to day activities, carry your APF ER Kit and Dr. Information, made of Quality construction and water resistant. Has APF Logo on it. 10.00 each
9. APF- Wristbands
100% Silicone Comes in Purple, Red/Purple, and Light Blue says: APF-PORPHYRIA
2/6.00
10. Womens Decorative Scarfs
Comes in Black, Purple, Red, Orange, Coral, Blue, and Lime. Many ways to where this dressy or everyday look. 8.00 each
11. EMTEC 16 GIG USB Drive
You cant go wrong with this handy dandy gadget. Store all your medical records, medication list, safe/unsafe APF Acute Drug List, Doctors Names and Address and Numbers Get smart and save some time. It comes in so handy in the Doctors office, ER whatever your need it for. Yellow with APF logo on Front 14.00$
12. All Furry Animals Lovers~ Kitty pillows with catnip
These handmade kitty pillows with all fresh natural catnip will keep your kitty happy every day. Handmade by an AIP patient. Dont forget your furry friend. 4/10/00 or 2.50 each
13. All Furry Animals Lovers~ Doggies Toys~ with squeakers
These handmade Doggie toys with squeaker have all natural fibers and plastic small squeaker. Your doggie needs love to, buy for a great cause. APF. 4.50 each
To make ONLY Cash, Credit Card donations follow this link. http://www.firstgiving.com/fundraiser/aapf/aapfsfundraisingpage via @firstgiving
How Sarah Lee is making a buzz about Porphyria Awareness week!
Here's a link to the American Porphyria Foundation in case you are wondering what in the world is Porphyria. :) I have been diagnosed since 1997. So many of you were in HS with me while I was "getting sick". That is when I started having symptoms but I was born with it. Remember me passing out in school & leaving by ambulance, having to quit sports teams I played on with you, being missing from classes a lot, in the nurses station all the time, having rapid weight gain? It was confusing & scary. I lost many friends who had never been exposed to someone with a chronic illness beforelet alone someone their own age having something they've never heard of. Some people, even those close to me, even accused me of "faking it" for attention. I do not blame them. People fear what they do not know. So this is a big reason I want to educate as many people about Porphyria as possible. I feel this applies to other things that may be unknown to the masses like other rare diseases, cancer, people with special needs or disabilities.
Don't be afraid, if you don't knowask instead of judging. And for those who are affected or have a loved one who is, don't be mad at others for reacting negativelyeducate them instead. It our responsibility to share and talk about it even if we are afraid being received negatively and judged. It is the only way to make things better. Be strong and know that you are not alone.
Thank you Sarah Lee for sharing your personal story of what you have went through and how you have overcome and managed Porphyria.
Remember.Research is the Key to your cure!
Clinical Studies: Whats in It for You?
Friday - April 12, 2013 @ 20:53:27
Clinical Studies: Whats in It for You? All porphyria patients and their families can contribute to medical knowledge of these diseases by volunteering for research. Each of the five Porphyria Clinical Research Consortium centers is recruiting patient volunteers with all types of porphyria. Participation could include treatment trials, or simply visiting a Consortium clinic. I have been lucky enough to take part in two clinical studies since my diagnosis with AIP in 1995. For me the most rewarding part of each project was the one-on-one time spent with a porphyria expert. As part of each study I was examined by, and discussed my history with, a doctor who had spent an entire career studying and treating the porphyrias. From a purely selfish point of view, I found it comforting to receive feedback on my experience with AIP, and advice about future treatment, from physicians who have seen more than a handful of cases. While I have always liked the doctors who care for me at my local hospital, speaking with an expert gave me added confidence that I am following the best course of treatment for me. There is also the greater good to be served by taking part in a study. Patients who volunteer for clinical research can be proud to know that they are adding to medical knowledge about porphyria, making it possible for other patients to receive better care. Understanding that porphyria is a family disease makes this easy for anyone to relate to. Mira Geffner~Porphyria patient
Remember.Research is the Key to your cure!
Read a story about Meghann Bauer with EPP
Thursday - April 11, 2013 @ 10:07:22
Meghann Bauer
Type of Porphyria:
Erythropoietic Protoporphyria (EPP)
Meghann Bauer has had symptoms of erythropoietic protoporphyria (EPP) since she was a little baby, yet her parents took her to different doctors for years before she was diagnosed at age 16 with EPP. Meghann says "I just never found the right way to describe my symptoms so that the doctors would think to test me for EPP," and she was tested for lupus and many other conditions before her diagnosis. It wasn't until her mother brought Meghann to her pediatrician's office saying that she had watched Meghann fall asleep on a family car trip, and that every time the sun hit Meghann's skin she flinched away from it or woke up in pain, that doctors began to suspect porphyria. Watching the Discovery Channel recently, Meghann found the story told in an episode of Mystery Diagnosis strikingly familiar. The show featured the Leppert family and their struggle to come up with an EPP diagnosis for their son Craig, and Meghann's family went through many of the same stages of misdiagnosis that the Leppert family did. Meghann says Craig Leppert's description of his EPP symptoms matches the feeling perfectly: "it's like putting your hand on a hot stove and then slicing your skin with a knife," a pain that is dull and steady and then suddenly sharp and searing. Meghann has memories from her childhood of running her hands under cold water to relieve the burning pain. She and her parents did not know it was dangerous for her to be out in the sun, so she was exposed throughout the summer and the season meant constant pain. She recalls falling asleep covered in ice packs every night, and her mother describes little Meghann as having been in such pain every night, and then finally, when the ice cooled her enough and she was simply exhausted, she would heave a big sigh and go to sleep. When she was very small, Meghann's doctors suggested she was allergic to PABA because every time her symptoms flared up she had been covered in a sunscreen containing PABA. No one realized the problem was the sun itself, not her parents' efforts to protect her. When her pediatricians could not find anything wrong with her, they even told Meghann's parents to take her to a psychiatrist for what they assumed were psychological problems. Luckily, the psychiatrist assured Meghann's parents that there was nothing wrong with their daughter emotionally and that something physical was clearly causing her pain. The dermatologist was surprised when tests came back positive, having said up front "you don't have EPP," something many porphyria patients have heard before. The thing about rare diseases is that while most people don't have them, some people do. And the people with those diseases are just as deserving of diagnosis and treatment as those with more common conditions. Diagnosis did not come til age 16. Yeesh! Since she was diagnosed, Meghann takes Lumitene to help with her symptoms. She takes 10-12 pills daily throughout the summer months, and fewer in winter. Although she still has some symptoms in the summer, she is usually symptom-free all winter, except when skiing or outdoors in snow country, where the reflected sunlight causes bad symptoms. When she does have flare-ups of her EPP symptoms, she uses motrin and darvocet for pain, and packs on ice. Meghann has also spoken with Dr. Micheline Mathews-Roth since her diagnosis, and has a genetic counselor who sees several other families in the area whose children have EPP. The genetic counselor is anxious to help and has also been in touch with Dr. Roth. Today, Meghann is a member of the APF and a patient looking forward to participating in clinical trials of Afamelanotide from Clinuvel. She is hopeful that this may be a way to "help my husband and I do the things we enjoy, such as boating, swimming in our pool, picnics, walking our boxer puppy."
National Porphyria Awareness Week
Wednesday - April 10, 2013 @ 17:15:18
National Porphyria Awareness Week
April 14-21, 2013
This is your opportunity to enhance Porphyria awareness in your community. Although the APF promotes porphyria awareness every day of the year, Porphyria Awareness Week presents us all with the opportunity to simultaneously flood the media, medical facilities, friends and family with information to help others understand more about Porphyria. The week can also be our reminder to promote some awareness activity throughout the year.
We are happy to report that many people have been diagnosed through your awareness efforts. Everyone has a story that can benefit others. If you would like materials to help you in your awareness project, please contact the APF.
Together we can improve porphyria diagnosis and treatment.
If you need materials or have any questions please contact the APF @ 1.866.APF.3635.
Share your campaign with us and others on the APF fb page.
"Remember.Research is the key to your cure!"
Are you joining and helping this year check out FB plans for Porphyria Awareness Week!
National Porphyria Awareness Week April 22-28, 2012 is all about YOU!
The challenge of living with Porphyria starts with how little is known about it among friends, family and the medical community. That is why National Porphyria Awareness Week is so important. It provides each of YOU with the opportunity to enhance Porphyria awareness among the public and medical professionals right where you live. Many of you helped last year, setting up at hospital Health Fairs, seminars and grand rounds, gaining newspaper and television interviews, exhibiting at conventions. Some members even created their own campaigns to advance Porphyria awareness, but we need more of you to:
*Tell your story to local media. Television, newspapers, community magazines are looking for human interest stories about people who have encountered a major illness and have undertaken the challenge to help others in a similar situation. LeAnn Cook facilitated a family interview in the local newsletter about the boys EPP struggles. The Fleegel family appeared in a documentary on EPP that aired recently.
*SHARE knowledge about Porphyria at your Doctors offices and local hospitals. You might suggest that they host a seminar or grand rounds on Porphyria. Some members have even set up an information table or exhibit at a health fair. Amy Chapman sold Porphyria Awareness wristbands and set up seminars for doctors in her home town and even on vacation in Bermuda. Joanna Floyd attended Health Fairs and sent emails about Porphyria to nearby hospitals. Nathan Carr provided educational material about Porphyria to his hospital's medical library.
*ASSIST at an upcoming medical convention to help educate physicians on Porphyria and/or ask your hospital or doctor if there is a local meeting where you can hand out materials. Lana Spoto, Janie Williams, Molly Buffington, Craig Humphries, Jessica Melton and her Dad, manned the exhibit booths at the Association for the Study of Liver Disease and American Society of Hematology medical conventions. You can do the same at this years meetings.
*VOLUNTEER your talents to help achieve the educational programs of the APF. Our talents are varied and plentiful and can be used to help one another. For example, you might want to donate one of your paintings, sculpture, weaving, etc. for our fall raffle. An anonymous donor sent the APF one of his paintings.
*VOLUNTEER your skills, like computer expertise, business acumen, or other skills to help achieve the educational programs of the APF. Computer expert, Rob Saupe, helped us with complex computer technical issues.
*HOLD a community race, car wash or other fund raising activity. Clarita Kimball and Lauren Warren raced in Night Runs to enhance Porphyria awareness. Wyatt King entered a Box Car race for Porphyria.
*HONOR your loved one with a gift to the APF for a birthday, anniversary, holiday or memorial gift, like Dr. Susan Engel did to honor Bill Kasper and Linda M Pisciotta to honor Dr. Rebecca Corley; Here is one of the most unique ways . Kate Ruby purchased 200 APF wrist bands to put in the favor baskets for each guest at her wedding to honor her aunt. More about the bride and groom and her aunt with Porphyria story in the June newsletter .
*WRITE a letter to your friends and family asking them to make a donation like, Ralph Gray or vote for your pet in the Pet Beauty Contest, which will advance Physician Education and add some fun to our lives.
The APF can help you accomplish this goal by providing materials for your project:
What is an Expert Doctor for the APF? Time Training Bio's Awards and Reading
Thursday - April 4, 2013 @ 09:48:05
Can you define what an "Expert" is? The meaning of an expert is having, involving, or displaying special skill or knowledge derived from training or experience. Why is this so important to know what this term means in modern day medicine? Many people today are rushed, have high anxiety, work, family and the list goes on. So "life" is already complicated. Now you add a rare disease to your list, now every thing changes in your life. You want to know all the answers right then and what to do, but its not easy with every one's opinions and what is right for you. So back to the term "Expert" & "Porphyria." Why have an Expert Porphyria Doctor from the American Porphyria Foundation? Aren't they just a normal MD? Let's share some valuable facts about these very Doctor's.
They have been featured in major medical Journals such as: Articles of Excellence, New England Journal of Medicine, Annals of Medicine
Has your Doctor ever written a major medical text books about your disease? What a privilege that the APF "Expert Doctors have! See below Bio's and Medical text books from them **
Are they known as Experts/Experienced with the (NIH)?
AKA~ National Institute of Health
Do you know if your Doctor has ever been involved with Major Research Projects? The APF Doctors have been involved with so many over the years. At this time we are IN NEED of VOLUNTEERS to sign up for studies, you can sign up below by clicking on this link: http://rarediseasesnetwork.epi.usf.edu/registry/direct.htm.
Has your Doctor attended many of the Porphyria Conferences, traveling through out all parts of the world speaking, teaching and sharing valuable knowledge?
Are they world renown among their peers in the field of Prophyria?
We even have an Scientific Advisory Board is made up of the world's foremost experts in porphyria management, diagnosis, and research. They have written or approved the medical information on this website.
We would love to share with you a few Bio's on these "Expert Porphyria Doctors", what extensive training they have achieved, the medical textbooks they have written, the studies and research programs and how they have been honored. We Thank each Doctor that has dedicated their time and life to help us those who struggle with Porphyria. We look forward to supporting our Programs called "Protect the Future" (PTF) in your donations to the APF to this cause to continue to finding these rare gems in the medical field.
Learn about:
Joseph Bloomer, MD, Professor, Liver Center Director
Dr. Bloomer is a Professor of Medicine and the Director of the UAB Liver Center at UAB. He received his medical degree from Western Reserve Medical School and completed his fellowship training in gastroenterology at Yale University. Dr. Bloomer is considered to the one of the leading experts in the treatment of hepatitis B and porphyria, and is world renowed for his research in genetic diseases of the liver. Since joining UAB in 1995 he has aided in the growth of services available to patients suffering from liver related diseases. Dr. Bloomer is active in the Faculty practice treating patients suffering from all liver related disorders. He is also active in both basic science and clinical research with a focus in liver disease, porphyria, genetics, and hepatitis B. He also has been honored with the highest award the Presidential Award among over 8,000 specialists.
Professor, Division of Gastroenterology and Hepatology
Karl E. Anderson, M.D. Professor of Preventive Medicine and Community Health Internal Medicine, and Pharmacology and Toxicology
University of Texas Medical Branch Bio
A graduate of the Johns Hopkins University School of Medicine, Dr. Anderson completed his residency and postgraduate training in gastroenterology at the New York Hospital-Cornell Medical Center. He was a member of the faculty at the Rockefeller University, Cornell University Medical College and New York Medical College before coming to UTMB in 1987. He directs the Division of Human Nutrition in the Department of Preventive Medicine and Community Health, and is an active clinical investigator particularly on the General Clinical Research Center (GCRC), where he is also Associate Program Director. He is PI for UTMB's NIH K30 grant that supports a variety of clinical research education programs, Director of the Clinical Research Education Office, and Director of the Graduate Program (PhD or MS) in Clinical Science, which is suited particularly for physicians seeking advanced training in clinical research.
Research Interests
Dr. Anderson's research interests include (i) pathogenesis of human porphyrias and identification of factors that increase susceptibility; (ii) development of new therapies for porphyrias; (iii) effects of diet on drug metabolism in humans, especially by cytochrome P450 enzymes, and on circulating hormone levels; (iv) collaborative work on effects of soy feeding in humans on breast cancer risk.
Clinical Interests
Dr. Anderson clinical interests include human porphyrias, metabolic and nutritional aspects of liver disease, and general clinical gastroenterology and hepatology.
Selected Publications
Egger NE, Goeger DE, Payne DA, Miskovsky EP, Weinman SA, Anderson KE. Porphyria cutanea tarda: multiplicity of risk factors including HFE mutations, hepatitis C and inherited uroporphyrinogen decarboxylase deficiency. Digestive Diseases and Sciences 2002; 47:419-426.
Anderson KE, Bloomer JR, Bonkovsky HL, Kushner JP, Pierach CA, Pimstone NR, Desnick RJ: Recommendations for the diagnosis and treatment of the acute porphyrias. Annals of Internal Medicine 2005;142:439-50.
Huang Y, Cao S, Nagamani M, Anderson KE, Grady J, Lu L-JW: Decreased circulating levels of tumor necrosis factor-alpha (TNF-a) in postmenopausal women during consumption of soy containing isoflavones. Journal of Clinical Endocrinology and Metabolism 2005;90:3956-62.
Nhan S, Anderson KE, Nagamani M, Grady JJ, Lu LJ: Effect of a soymilk supplement containing isoflavones on urinary f2 isoprostane levels in premenopausal women. Nutrition and Cancer 2005;53(1):73-81.
Akagi R, Kato N, Inoue R, Anderson KE, Jaffe EK, Sassa S: delta-Aminolevulinate dehydratase (ALAD) porphyria: The first case in North America with two novel ALAD mutations. Molecular Genetics and Metabolism. 2006:87:329-336.
Akagi R, Inoue R, Muranaka S, Tahara T, Taketani S, Anderson KE, Phillips JD, Sassa S. Dual gene defects involving d-aminolaevulinate dehydratase and coproporphyrinogen oxidase in a porphyria patient. British Journal of Haematology. 2006;132:237-243.
Anderson KE, Collins S. Open-label study of hemin for acute porphyria: clinical practice implications. American Journal of Medicine. 2006;119:19-24.
Anderson KE: The porphyrias (Chapter 72), in Boyer T, Wright T, Manns M (eds): Zakim and Boyer's Hepatology: A Textbook of Liver Diseases. Philadelphia, Elsevier, 2006, pp 1391-1432. 9.
Anderson KE, Porphyria cutanea tarda Ã?¢â¬ââ?¬Å? a possible role for ascorbic acid (Editorial) Hepatology, 2007;45(1):6-8. 10.
Madan P, Schaaf CP, Vardhan P, Bhayana S, Chandra P, Anderson KE: Hans Gunther and his disease. Photodermatol Photoimmunol Photomed 2007;23(6):261-3.
Desnick RJ, Astrin KH, Anderson KE. Heme biosynthesis and the porphyrias (Chapter 28). In: Suchy, FJ, Sokol, R,J, Balistreri, WF, eds. Liver Disease in Children, 3rd edition. Cambridge: Cambridge University Press, 2007, pp 677-693.
Anderson KE. The porphyrias (Chapter 223). In: L. Goldman and D. Ausiello., eds. Cecil Textbook of Medicine, 23rd edition, Philadelphia, W.B. Saunders Co., 2007, pp 1585-1593.
Desnick is the Dean for Genetics and Genomics, Interim Director of the Mount Sinai Genomics Institute, and Professor and Chair of the Department of Genetics & Genomic Sciences at TheMount Sinai School of MedicineinNew York City. Additionally, he is Physician-in-Chief of the Department of Medical Genetics and Genomics at TheMount Sinai Hospital.
Desnick is the author of more than 600 peer-reviewed articles in scientific journals, 200 book chapters and is the editor of nine books. He holds 13 patentsand is included inCastle Connelly's lists of Best Doctors in America and Best Doctors in New York andNew York Magazines list of the Best Doctors every year since the inception of the rating.He was elected to theInstitute of Medicinein 2004.
Desnick received his undergraduate degree from theUniversity of Minnesotain 1965. He earned a Ph.D. in genetics from the University of Minnesota Graduate School in 1970 and his M.D. from theUniversity of Minnesota Medical Schoolin 1971. He completed an internship and a residency in pediatrics at theUniversity of Minnesota Hospitalsand joined the faculty at the University of Minnesota, where he rose to the rank of Associate Professor of Cell Biology and Genetics and Pediatrics.Biography
Desnick joined the staff at Mount Sinai Medical Center in 1977, as the Arthur J. and Nellie Z. Cohen Professor of Pediatrics and Genetics and Chief of the Division of Medical and Molecular Genetics in the Department of Pediatrics. He was the first Chairman of the newly-created Department of Human Genetics in 1993, which was renamed the Department of Genetics & Genomic Sciences in 2006. In 2009, he became Dean for Genetics & Geonomics and Interim Director of the newly established Genomics Institute at Mount Sinai. He is currently Professor of Pediatrics, Oncological Sciences, Obstetrics, Gynecology and Reproductive Science, Gene and Cell Medicine and Professor and Chair of Genetics & Genomic Sciences.
Desnick is a past director of theAmerican Board of Medical Genetics, a Founding Diplomat of theAmerican College of Medical Genetics, a past member of the board of directors of the American College of Medical Genetics Foundation, and a founder and past-president of the Association of Professors of Human and Medical Genetics.He is past chair of theAssociation of American Medical Colleges(AAMC), past member of the AAMC Board of Directors and past chair of the AAMC Council of Academic Societies.
Fellowships and awards:
Partial list:
·U.S. Public Health Service Fellowship in Genetics, 19681970
·Ross Award in Pediatric Research, 1972
·C.J. Watson Award, University of Minnesota, 1973
·NIH Research Career Development Award, 19751980
·E. Mead Johnson Award for Research in Pediatrics of the American Academy of Pediatrics, 1981
·Honorary Member, Japanese Society for Inherited Metabolic Diseases, Elected 1985
·Correspondent Member, Societá Italiana di Pediatria, Elected 1991
·Honorary Member, Societá Italiana di Pediatria, Elected 1999
·Outstanding Faculty Award, Mount Sinai School of Medicine, 1991
·NIH MERIT Award, 19922004
·J. Lester Gabrilove Award for Medical Research, 2003
·Jacobi Medal, Mount Sinai Alumni Association, 2004
·Edward H. Ahrens, Jr. Award for Research from the Association for Patient-Oriented Research, 2004
·University of Minnesota Medical School Distinguished Alumni Award, 2004
·Doctor of Science, Honoris Causa, Mount Sinai School of Medicine of New York University, 2004
·Porphyrias and Human Heme Biosynthesis, National Institute of Diabetes and Digestive and Kidney Diseases
·Alpha Galactosidases A And B -- Molecular and Cellular Mechanisms, National Institute of Diabetes and Digestive and Kidney Diseases
·Gene Therapy: Lysosomal Diseases With Mental Retardation, National Institute of Child Health & Human Development
Patents
Patent No.
Title
6,583,158
Method for enhancing mutant enzyme activities in lysosomal storage disorders
6,541,218
Acid sphingomyelinase protein and methods of treating type B Niemann-Pick disease
6,455,037
Cells expressing an .alpha.gala nucleic acid and methods of xenotransplantation
5,840,578
Methods for determining susceptibility to lead poisoning
5,830,850
Methods for the treatment of bone resorption disorders, including osteoporosis
5,773,278
Acid sphingomyelinase gene
5,686,240
Acid sphingomyelinase gene and diagnosis of Niemann-Pick disease
5,639,607
Method and kits for detecting a polymorphism in delta.-aminolevulinate dehydratase gene which is associated with an altered susceptibility to lead poisoning
5,580,757
Cloning and expression of biologically active alpha-galactosidase A as a fusion protein
5,491,075
Cloning and expression of biologically active alpha N-acetylgalactosaminidase
5,401,650
Cloning and expression of biologically active alpha-galactosidase A
5,382,524
Cloning and expression of biologically active alpha-N-acetylgalactosaminidase
5,356,804
Cloning and expression of biologically active human alpha-galactosidase A
·Desnick, R.J., Bernlohr, R.W. and Krivit, W., eds.:Enzyme Therapy in Genetic Diseases, Birth Defects Original Article Series. Vol. IX, No. 2.The National Foundation, New York, pp. 236, 1973.ISBN 0-683-06367-7
·Rubenstein, I., Phillips, R.L., Green, C.E. and Desnick, R.J., eds.:Molecular Genetic Modification of Eucaryotes, Academic Press, New York, pp. 171, 1977. ASIN B000N5X2F2
·Desnick, R.J., ed.:Enzyme Therapy in Genetic Diseases: 2, Alan R. Liss, Inc., New York, pp. 544, 1980.ISBN 0-8451-1035-7
·Desnick, R.J., Patterson, D.F. and Scarpelli, D.F., eds.:Animal Models of Inherited Metabolic Diseases.Alan R. Liss, Inc., New York, pp. 519, 1982. ASIN B0028IQ4KC
·Desnick, R.J., Gatt, S. and Grabowski, G.A., eds.:Gaucher Disease: A Century of Delineation and Research, Alan R. Liss, Inc., New York, pp. 740, 1982.ISBN 0-8451-0095-5
·Bishop, D.F. and Desnick, R.J., eds.:Assays of the Heme Biosynthetic Enzymes.Enzyme 28:1-232, 1982.ISBN 978-3-8055-3573-1
·Tada, K., Colombo, J.P. and Desnick, R.J., eds.:Recent Advances in Inborn Errors of Metabolism.Karger, Basel, pp. 332, 1987.ISBN 3-8055-4772-2
·Desnick, R.J., ed.:Treatment of Genetic Diseases, Churchill Livingstone, Inc., New York, pp. 331, 1991.ISBN 0-443-08773-3
·Ziegler, RJ, Cherry, M, Barbon, CM, Li, C, Bercury, SD, Armentano, D, Desnick, RJ, Cheng, SH: Correction of the biochemical and functional deficits in Fabry mice following AAV8-mediated hepatic expression of alpha-galactosidase A Mol. Ther. 15:492-500, 2007.PMID 17191071
·Germain, DP, Waldek, S, Banikazemi, M, Bushinsky, DA, Charrow, J, Desnick, RJ, Lee, P, Loew, T, Vedder, AC, Abichandani, R, Wilcox, WR, and Guffon, N: Sustained, long-term renal stabilization after 54 months of agalsidase beta therapy in patients with Fabry disease J. Am. Soc. Nephrol. 18:1547-1557, 2007.PMID 17409312
·Grace, ME, Balwani, M, Nazarenko, I, Prakash-Cheng, A, and Desnick, RJ: Type 1 Gaucher disease: Null and hypomorphic novel chitotriosidase mutations- implications for diagnosis and therapeutic monitoring. Hum. Mut. 28:866-873, 2007.PMID 17464953
·Scott, SA, Edelmann, L, Kornreich, R, Erazo, M and Desnick, RJ: CYP2C9, CYP2C19, and CYP2D6 allele frequencies in the Ashkenazi Jewish population. Pharmacogenomics 8:721-730, 2007.PMID 18240905
·Yasuda, M, Domaradzki, M, Bishop, DF, and Desnick, RJ: Acute intermittent porphyria: Vector optimization for gene therapy J. Gene Med. 9:806-911, 2007.PMID 17654633
·Cunha, L, Kuti, M, Bishop, DF, Mezei, M, Zeng, L, Zhou, MM and Desnick, RJ: Human uroporphyrinogen III synthase: NMR-based mapping of the active site. Proteins 71:855-873, 2008.PMID 18004775
·Scott, SA, Edelmann, L, Kornreich, R and Desnick, RJ: Warfarin pharmacogenetics: CYP2C9 and VKORC1 genotype predict different sensitivities and resistance frequencies in the Ashkenazi and Sephardi Jewish populations. Am. J. Hum. Genet. 82:495-500, 2008.PMID 18252229
·McGovern, MM, Wasserstein, MP, Giugliani, R, Bembi, B, Vanier, M, Mengel, E, Brodie, SE, Mendelson, D, Skloot, G, Schuchman, EH Kuriyama, N, Desnick, RJ, and Cox, GF: A prospective, crosssectional survey study of the natural history of Niemann-Pick disease Type B. Pediatrics 122: e341-349, 2008.PMID 18625664
·Schiffmann, R, Banikazemi, M, Bultas, J, Linthorst, GE, Packman, S, Warnock, D, Asger Sorensen, S, Wilcox, WR, and Desnick, RJ: Fabry disease: progression of nephropathy, and prevalence of cardiac and cerebrovascular events before enzyme replacement therapy Nephrol. Dial. Transplant. 24:2102-2111, 2009.PMID 19218538
·Benjamin, ER, Flanagan, JJ, Schilling, A, Chang, HH, Agarwal, L, Datz, E, Wu, X, Pine, C, Wustman, B, Desnick, RJ, Lockhart, DJ, and Valenzano, KJ: The pharmacological chaperone 1-deoxygalactonojirimycin increases α-galactosidase A levels in Fabry patient cell lines. J. Inherit. Dis. 3:424-440, 2009.PMID 19387866
·Hwu, WL, Chien, YH, Lee, NC, Chiang, SC, Huang, AC, Yeh, HY, Chao, MC, Lin, SJ, Kitagawa, T, Hse, LW, Desnick, RJ, and Hsu, LW: Newborn screening for Fabry disease in Taiwan reveals a high incidence of the later-onset mutation, IVS4+919G>A. Hum. Mutat., June 26, 2009.PMID 19621417
·Scott, SA, Jaremko, M, Lubitz, S, Halperin, JL, Desnick, RJ: CYP2C9*8 is prevalent in African-Americans: implications for pharmacogenetic dosing. Pharmacogenomics 10:1243-1255, 2009.PMID 1963669
·Galende, E., Karakikes, I, Edelmann, L, Desnick, RJ, Kerenyi, T, Khoueiry, G, Lafferty, J, McGinn, JT, Brodman, M,Fuster, V, Hajjar, RJ, and Polgar, K Amniotic fluid cells are more efficiently reprogrammed to pluripotency than adult cells. Cloning Stem Cells [Epub] Dec. 17, 2009.PMID 20017623
·Khanna, R, Soska, R, Lun, Y, Feng, J, Frascella, M, Young, B, Brignol, N, Pellegrino, L, Sitaraman, SA, Desnick, RJ, Benjamin, ER, Lockhart, DJ and Valenzano, KJ: The pharmacological chaperone 1-deoxygalactonojirimycin reduces tissue globotriaosylceramide levels in a mouse model of Fabry disease. Mol. Ther. 18:23-33, 2010.PMID 19773742
·Yasuda, M, Bishop, DF, Gan, L, Fowkes, M, Ziegler, R, Cheng, SH, and Desnick, RJ: AAV8-mediated gene therapy prevents induced biochemical attacks of acute intermittent porphyria. Mol. Ther. 18:17-22, 2010.PMID 19861948
·Wozniak, M, Kittner, S, Tuhrim, S, Cole, J, Stern, B, Dobbins, M, Grace, M, Nazarenko, I, Dobrovolny, R, McDade, E, Desnick, RJ: Frequency of unrecognized Fabry disease among young European-American and African-American men with first ischemic stroke. Stroke 41: 78-81, 2010.PMID 20007919
We hope that you could see just a glimpse of these wonderful Doctors why it is so important to educate your self, your family and your Doctors about Porphyria, getting the facts about testing, diagnosing and treatment with an Expert APF Doctor. Please feel free to print or save this document if you have any additional questions please contact the American Porphyria Foundation @ 866-apf-3635 or visit www.porphyriafoundation.com to ask how you can get a complete listing detail in Doctors in your area.
Remember.Research is the Key to your cure!
Early Bird Registration Porphyria Patient Day Lucerne: End of March!
The date for the third International Porphyria Patient Day in Lucerne on May 18th is rapidly approaching and we kindly want to remind you about the deadline for early bird registration at the end of March. From April 2nd on, the registration fee will increase significantly.
We welcome you to share your experience, strengthen your network and benefit from direct contact to international porphyria experts! We already have participants registered from all over the world so dont miss the opportunity to be part of this unique event!
Exciting news : Over the next six months, renowned porphyria specialist, Dr Karl Anderson, will be traveling around the country to register patients for the Registry research projects and the Longitudinal Study right in your own home town.
Here is what we need you to do, if you have not joined the The APF, please do so immediately. It does not cost anything to join although donations are always appreciated. We need a means to locate where people with porphyria are living. For example, we know there are patients in the middle of Florida and Southern Florida so we want to set up for a few days there. Without your names and type of porphyria we will not know where is best to place Dr Anderson's traveling. Research unit .
All porphyrias are needed, so please join ASAP. We will begin mapping the cities to visit next week.
"We would like to thank all of our Members and Supporters. The APF is our Members. We are very blessed to have so many wonderful people helping us to educate and train Doctors for our Porphyria care. We would like to take a minute and apologize for any confusion about the Suggested Donation for APF Membership. There was a problem with the website and the changes to the Join the APF form had been lost. The problem has now been corrected. There is no fee for membership to the APF. There is a suggested donation for membership because the APF runs on donations. The website, Educational materials for you and your Doctors are just a few of the many things that the APF does.
Your donations can also go to specific projects if you choose.
Maybe finances wont allow you to donate Money. If you would like to donate your time there are always ways to assist us with the many ongoing projects. If interested Contact us at porphyrus@aol.com.
Important news..Read all about it be informed and support the APF
Tuesday - April 2, 2013 @ 12:55:45
Important news..
Porphyria Awareness Week!
The Annual National Porphyria Awareness week will be held April 14th-20th 2013.
Bringing awareness to our communities, medical providers and loved ones starts with YOU.
In years past, we have had members contact their local media to do an interview or suggest an idea for a story about porphyria. Others have held events like hikes, races, medical fairs and presentations on porphyria.
Our young members have been especially creative including their schools in their awareness activities. The Cook brothers are hosting Hat Day again this year in their community schools. Everyone wears a hat and brings a dollar to promote EPP awareness and its photosensitivity, as well as raise funds for the APF.
Even bringing educational materials to your doctor's offices is a very important effort.
No matter how big or small your activity, you can enhance porphyria awareness every week of the year. But Porphyria Awareness Week is a great time to start. The APF is all of us and this week gives us the opportunity to educate physicians and the public about porphyria.
If you need help with ideas or educational materials please contact the APF office. 1.866.APF.3635 .
Join the Porphyria Registry.
The Porphyria Consortium needs more Porphyria patients and their families to join the Porphyria Registry to be able to receive the Government funds to continue their present and future research projects.
Ongoing Research projects include:
Longitudinal study of all the Porphyrias.
Recurring attacks in the Acute Porphyrias.
Erythropoietic Protoporphyrias: Studies of the Natural History, Genotype-Phenotype Correlations, and Psychosocial Impact (7207).
Amanpal Singh, MD, MS is one of our newet Protect the Future (PTF) doctors training with porphyria specialist, Dr. Karl Anderson. Dr. Singh is a Gastroenterology and Liver expert at University of Texas Medical Branch, Galveston, Texas where he serves as the Chief Fellow, in the Department of Gastroenterology. After finishing medical school at the most prestigious institution in India, All India Institute of Medical Sciences, he received a Masters degree in Epidemiology from Harvard University. Currently, Dr. Singh is collaborating with Dr. Karl Anderson to study the epidemiology of porphyrias and patterns of care for porphyria patients in the United States using claims based database. He brings his wide experience working with large databases, like the national Medicare claims database, to help determine baseline data on the burden of disease and quality of care that porphyria patients receive. Dr. Singh is also managing porphyria patients with Dr. Anderson. Porphyria patients travel to the Texas Porphyria Center from around the nation and even internationally to seek expert care for their particular type of porphyria. They come for diagnosis and treatment, thus, giving Dr. Singh clinical experience in all types of porphyria. In either case, most of the patients have endured a host of tests without receiving a diagnosis and are very grateful when they receive a diagnosis at UTMB. Aside from his main medical interests, Dr. Singh is involved in performing comparative effectiveness research and health services research and has accumulated an extensive list of peer reviewed publications and presentations Dr. Singh recently attended the PTF Training Week with other PTF doctors at the UTMB Porphyria Center. We are grateful that he will be counted among the future experts. We are proud to have a physician of Dr. Singhs caliber. WELCOME !!!!!!!
February 28 is Rare Disease Day a concept first initiated by the European Rare Disease Organization (EURORDIS) and now recognized around the world. Around 6,800 rare diseases have been identified and up to 80% of them have a genetic origin. 23andMe provides genetic health reports for many of these conditions and also carries out research on a few of them.
When it comes to rare diseases, rare is not actually that rare.
Take that one person with cystic fibrosis, the other person with sarcoma, and then someone with sickle cell anemia. All of these conditions are considered rare, but when you add up all the people with a rare disease you land at one in ten. This means that roughly 30 million Americans suffer from a rare disease.
Definitions can vary, but in the United States the rare label is applied to any condition that affects fewer than 200,000 individuals, or roughly one in 1500. Rare diseases are often poorly understood, with symptoms that can be difficult to diagnose, and can be life-threatening.
Most rare diseases cant be cured and many lack effective treatments because research is often hampered by a scarcity of study participants and poor funding. 23andMe hopes to change this.
Our Myeloproliferative Neoplasms and Sarcoma research initiatives are aimed at understanding what causes these conditions, information that may one day help bring about a cure.
Beyond these initiatives we also research rare diseases through the typical customer experience. Individuals come to 23andMe, receive their genetic results, and if they desire, contribute to research by providing information about themselves. Our scientists aggregate this information and draw interesting correlations.
A first-glance finding is that roughly nine percent of 23andMe customers have a rare disease, right on par with the national average of ten percent. Slightly more 23andMe individuals with a rare disease are women.
As soon as I woke up today, I knew it was going to be a day where I decided to take a break from lifes duties. Around noon, I started to feel a little guilty and my shame button was triggered. If I sit down and rest, Im being lazy said my negative self-talk.
I took a look at my activities over the past week, packed with work, appointments and other commitments. As I neared the end of the week, I could feel the life being sucked out of me. I was struggling to keep my symptoms tame.
Sometimes I feel like I just dont have any fight left in me, but I still have a hard time resting. I think this is partly due to my personality (Im much more like the hare than the tortoise), and partly due to our over-achiever syndrome culture here in America. The How to Cope with Pain article Making Positive Psychological Changes talks about acceptance and how it can mean no longer struggling with the pain. Ive come to a point in my journey where I do accept my pain (most days) and today was a good example of this. I realized that a) Im exhausted, and b) I have an increase in symptoms. So, Im not being lazy! In fact Im doing something good! Im resting and using some tools to manage my symptoms of chronic pain.
But how did I get to this point? Here are a couple things I do to make sure I stop and insert the rest that I need, when I need it:
1. Stop Sign!
When I start to get down on myself for fear of being lazy, I need to just STOP. Stop my thoughts (those squirrels and monkeys in my head) and be where my hands are.
2. What do I need?
A good question to ask ourselves! What is it that I need at this very moment? It could be some or all of the following: rest, stretching, food (the healthy kind of course), movie, friend, nap, good cry, nature, or connection with a Higher Power.
3. Satisfy the need
Now that weve determined what it is that we need, lets engage and get our needs met in a healthy and effective manner. For instance, what my body needed today was rest, relaxation, healthy/nourishing food, and some restorative yoga.
4. Be gentle
This is not a No Pain, No Gain situation. We need to give ourselves grace and forgiveness. The concept of self-love also falls under this. Many of us with chronic pain can easily keep pushing ourselves when we should not. We do this even though we know it can possibly increase our pain into a flare-up. Its okay to take a break when we need one, so give yourself permission to do so! Take care of you!
Are there days when you feel like youre being lazy even though you know deep down that resting is the right thing to do? How do you overcome the feeling of guilt? How do you allow yourself to take time to take care of yourself? Please share your thoughts in the comments!
Remember.Research is the Key to your cure!
Aubrey N Brooks and CEP
Thursday - March 28, 2013 @ 23:41:41
This website is for Aubrey Nichole Brooks
Before Transplant!
Now!
Aubrey was born on January 17th, 2008 to Nichole Baughman of Powhatan Point, Ohio. She was a healthy 8lbs. 13oz baby girl. Several weeks after she was born we noticed her diapers were tinted reddish-orange from her urine. After visiting the pediatrician and completing a urinalysis we were told she was fine. Throughout her first year of life she continued to have reddish-orange urine and the doctors assured us that everything was okay. She was admitted for pneumonia in March 2009 and the nurses showed a concern about her urine. They again did a urinalysis which came back negative. However, she was found to be anemic during this stay in the hospital. From March to June she began to show signs of blistering and scabbing on her face. This then spread to her hands and she began to lose her fingernails. We were misdiagnosed and were treated for impetigo for almost three months. In early June of 2009, we were seen by Dr. Robin Gehris who made her diagnosis. We were informed that she has a rare genetic disease called Congenital Erythropoietic Porphyria (CEP), also known as Gunther's disease. There has been under 200 cases of CEP reported worldwide. As far as we know there are only 8 persons living with this today. Aubrey cannot go outside to play in the daylight because of her disease. This disease causes:
extreme photosensitivity to sunlight and fluorescent bulbs
blisters on her hands and face, which burst and scar
enlarged spleen
liver and kidney failure
inability to go outside
intense pain
Due to Aubrey's condition we are having special windows installed in our home by Amerinat Builders. They block 95.4 % of the UV rays. We also had special window tinting put on our vehicles by C & L Window Tintingand the folks at Made in the Shadefound the yellow tint she also needed. This will hopefully help her from getting breakouts. Over time sun exposure will cause her to lose the tip of her nose, ears, and fingers. In addition, CEP can cause blindness, organ failure, and a shorten life expectancy. It is imperative that Aubrey wear 100 SPF sunscreen and sun protective clothing at all times.
Here is a link for information on all eight types of porphyria from The American Porphyria Foundation. Here is also a link to a great person who helped me with her sun protective clothing UV SUNGEAR. Also, Colleen at Fun Sunwear has make lots of Aubrey's clothing. You can also follow her progress by reading Aubrey's Updates throughout this experience. Nicholas Ashbyhas been cured by a bone marrow transplant. To read his story click on his name.
We found out Aubrey's genetic testing results from Mt. Sinai. They found that she has two mutations. One mutation from each parent. Doug and I are both carriers of this disease. They have done testing on Abbagayle to see if she is a match for Aubrey. I banked Abby's cord blood and they could have used that for Aubrey's transplant. Unfortunately, Abby is not her sisters keeper.
Aubrey was admitted to Children's Hospital of Pittsburgh of UPMC on January 11, 2010. She had a stem cell transplant on January 21, 2010. The donor was a 7 out of 8 match. She is doing well and to stay updated on her progress throughout this experience read her blog by clicking on Aubrey's Updates! Please keep her in your prayers. God Bless you and your family.
GREAT DREAM. Ten Keys to Happier Living
Thursday - March 28, 2013 @ 23:39:09
GREAT DREAM. Ten Keys to Happier Living
Feeling pain!
Thursday - March 28, 2013 @ 23:35:14
Pain provides the body with a protective mechanism, alerting it to potential or actual damage to the bodys tissues. In the example of a bee sting, the pain receptors in the skin detect tissue damage from the bee sting. Then, the peripheral nerves send a pain signal to the brain. The brain analyzes the pain signal. In turn, the brain delivers a message back to the muscles of the arm to react.
What is pain?
Thursday - March 28, 2013 @ 11:14:43
Pain is a feeling triggered in the nervous system. Pain may be sharp or dull. It may come and go, or it may be constant. You may feel pain in one area of your body, such as your back, abdomen or chest or you may feel pain all over, such as when your muscles ache from the flu.
Pain can be helpful in diagnosing a problem. Without pain, you might seriously hurt yourself without knowing it, or you might not realize you have a medical problem that needs treatment. Once you take care of the problem, pain usually goes away. However, sometimes pain goes on for weeks, months or even years. This is calledchronic pain. Sometimes chronic pain is due to an ongoing cause, such as cancer or arthritis. Sometimes the cause is unknown.
Fortunately, there are many ways to treat pain. Treatment varies depending on the cause of pain. Pain relievers, acupuncture and sometimes surgery are helpful. I hope your all having a pain free day.
Rafael de la Torre and PCT
Thursday - March 28, 2013 @ 11:05:23
Rafael de la Torre
Type of Porphyria:
Porphyria Cutanea Tarda (PCT)
Porphyria friends in Argentina have a center for diagnosis and treatment headed by Dr. Alcira Batlle. For more information , please see: http://www.qb.fcen.uba.ar/cipyp/
Our member, Rafael de la Torre from Buenos Aires shares his experience with PCT.
To contact him, email: rdelatorreu@hotmail.com In 2001 I went to consult the dermatologist about some blisters that appeared in one of my fingers. After asking me about others symptoms, he asked me to have an analysis performed by Dr. Alcira Batlle at the hospital in Buenos Aires. The result was Porphiria Cutanea Tarda. The treatment was S-Adenosyl-L-Methione, 800 mg/ day, during 20 days, and simultaneously I received 100 mg Chloroquine, twice a week, until the levels of urinary porphyrins reached the controls. And I also had one Phlebotony of 500 ml of blood. The concentration of urinary porphyrins and plasma porphyrins was measured at the beginning of the treatment and then every week, during therapy. When normal levels were reached, chloroquine intake was suspended. Clinical recovery was paralleled with biochemical recovery. I have regular controls performed every year, and since then I have been fine, without any relapse. With the porphiria diagnosis I went back to the dermatologist, and he told me that I have to consult one hepatologist, because I could have some liver damage. I did have, I had hepatitis C. I followed the treatment for about nine months with a combination of pills and Interpheron injections. At the end of this treatment, thanks God, I was healed. Nowadays, I have controls performed every year for this disease, too.
Remember.Research is the Key to your cure!
Quote for the Day
Wednesday - March 27, 2013 @ 19:22:43
" The happiest people don't have the best of everything, they just make the best of everything"
I do my best to live my life by this quote!
From an AIP suffer.
Remember.Research is the Key to your cure!
Peripheral Neuropathy~ Do you suffer?
Monday - March 25, 2013 @ 17:49:01
I know that many that suffer from Porphyria and other diseases also suffer from Peripheral Neuropathy. Learning about what it is how it affects us and what can we do to control our pain. This information has been provided by the Pain Management Clinic at the Mayo Clinic.
Peripheral neuropathy, a result of nerve damage, often causes numbness and pain in your hands and feet. People typically describe the pain of peripheral neuropathy as tingling or burning, while they may compare the loss of sensation to the feeling of wearing a thin stocking or glove.
Peripheral neuropathy can result from problems such as traumatic injuries, infections, metabolic problems and exposure to toxins. One of the most common causes is diabetes.
In many cases, peripheral neuropathy symptoms improve with time especially if the condition is caused by an underlying condition that can be treated. A number of medications often are used to reduce the painful symptoms of peripheral neuropathy.
Definition
Bottom of Form
Peripheral neuropathy, a result of nerve damage, often causes numbness and pain in your hands and feet. People typically describe the pain of peripheral neuropathy as tingling or burning, while they may compare the loss of sensation to the feeling of wearing a thin stocking or glove.
Peripheral neuropathy can result from problems such as traumatic injuries, infections, metabolic problems and exposure to toxins. One of the most common causes is diabetes.
In many cases, peripheral neuropathy symptoms improve with time especially if the condition is caused by an underlying condition that can be treated. A number of medications often are used to reduce the painful symptoms of peripheral neuropathy.
Symptoms
Bottom of Form
The nerves of your peripheral nervous system send information from your brain and spinal cord (central nervous system) to all other parts of your body and back again. Nerves that may be affected by peripheral neuropathy include:
·Sensory nerves that receive sensations such as heat, pain or touch
·Motor nerves that control how your muscles move
·Autonomic nerves that control functions such as blood pressure, heart rate, digestion and bladder function
Most commonly, peripheral neuropathy starts in the longest nerves the ones that reach to your toes. Symptoms vary, depending on which types of nerves are affected. Signs and symptoms may include:
·Gradual onset of numbness and tingling in your feet or hands, which may spread upward into your legs and arms
·Burning pain
·Sharp, jabbing or electric-like pain
·Extreme sensitivity to touch, even light touch
·Lack of coordination
·Muscle weakness or paralysis if motor nerves are affected
·Bowel or bladder problems if autonomic nerves are affected
Peripheral neuropathy may affect one nerve (mononeuropathy), two or more nerves in different areas (multiple mononeuropathy) or many nerves (polyneuropathy).
When to see a doctor Seek medical care right away if you notice any unusual tingling, weakness or pain in your hands or feet. Early diagnosis and treatment offers the best chance for controlling your symptoms and preventing further damage to your peripheral nerves. If your symptoms interfere with your sleep or you feel depressed, your doctor or pain specialist may be able to suggest treatments that can help. Please have your Doctor check with the APF safe/unsafe list for any Drug interactions. You can click on this link: http://www.porphyriafoundation.com/testing-and-treatment/drug-safety-in-acute-porphyria
Please JOIN: Connecting Patients Globally Its Free
Learn what it's like to live with a rare disease or share your own story. Browse patient testimonies, share photos, and contact patient organizations. The Understand section of RareConnect promotes awareness and understanding through daily life experiences.
·Meet
Start your global conversation here. Connect with others around the world to share support and encouragement. The Meet section of RareConnect provides a safe place to meet friends, ask questions, start or join conversations, and interact with others experiencing the same challenges.
·Learn
Find quality information from trusted sources. Read publications from medical experts and patient organizations. The Learn section of RareConnect links to FAQs, published articles, upcoming events, and other documents providing the latest information for each disease-specific community.
·Connect with others who understand
·Remember.Research is the Key to your cure!
Join up its FREEâ?¦..
www.rareconnect.org
MONICA'S PORPHYRIA AWARENESS WEEK EVENT
Sunday - March 24, 2013 @ 20:11:49
MONICA'S PORPHYRIA AWARENESS WEEK EVENT
We are excited about all of the activities our members are planning for the soon approaching Porphyria Awareness Week, April 14-20 2013. APF member, Monica Fleegel, is hosting a very creative campaign to heighten porphyria awareness and raise funds for the APF to train future experts via the Protect the Future program. The attendees will also be writing letters to the FDA in support of the approval of new treatments for EPP, like SCENESSE.
Read Monica's account below:
"Last summer, due to the tireless efforts of the APF, I was able to participate in Phase III clinical trials that gave me relief from the pain of EPP (Erythropoietic Protoporhyria). For the first time in my life, I spent time in the sun with my family and friends!! The APF was able to convince the FDA of the importance of continuing the trials and now we need to inform the FDA that we need a treatment so all who suffer from EPP can spend time in the sun. Through a letter writing campaign and your donations, we can assist the APF with this major endeavor. I am expecting up to 75 people at the fundraiser. If I can get even half to write letters wouldn't that be awesome? My friends and family loved being in the sun with me after 52 years of me being inside, so they want treatments like SCENESSE for EPP approved!"
Donating through this website page is simple, fast and totally secure. It is also the most efficient way to support Monica's fundraising efforts. Many thanks for your support -- and don't forget to forward this to anyone who you think might want to donate too!"
We hope you will choose an awareness activity. It may be as simple as bringing your Panhematin brochure to your doctors or taking the ER guidelines to your ER. Some people have approached their local media to do a story on their cases of porphyria. Watch next week for the Cook families event, HAT DAY, which will take place in all the schools in their town for PORPHYRIA AWARENESS WEEK.
"Remember.. Research is the key to your cure!"
Longitudinal Study Underway The Porphyria Longitudinal Observational Research Project
Sunday - March 24, 2013 @ 19:59:10
Longitudinal Study Underway The Porphyria Longitudinal Observational Research Project is underway. The objective of this protocol is to conduct a five year, multidisciplinary investigation of the natural history, morbidity, and mortality in people with porphyrias. In addition, the purpose is a long-term follow-up study of a large group of patients with the various porphyrias, which will provide a better understanding of the natural history of these disorders, as affected by available therapies, and to aid in developing new forms of treatment. You have the opportunity to be part of this important project and help advance research by answering the most important and often perplexing questions about porphyria. As part of the research, the patient volunteers will be followed longitudinally for long term survival, development of disease complications and outcomes of commonly used treatments, as well as more advanced treatments, such as liver or bone marrow transplantation. Researchers will seek to identify biochemical features (biomarkers) that may predict future symptomatic episodes so that interventions can be initiated before symptoms develop. The patients enrolled in this study will also be a source for other studies, including mechanistic investigations and clinical trials. The questions researchers want answered include: a.) In a longitudinal cohort, what is the prevalence of specific morbid indicators of disease severity, including neurovisceral and cutaneous manifestations, levels of porphyrin precursors and porphyrins, quality of life, long term effects on the liver, kidneys and other tissues, and case-fatality associated with the various forms of porphyria? b.) What are the relationships between disease severity and progression and various biomarkers-biological characteristics, such as genotypes, causative and contributing endogenous and environmental factors and levels of porphyrin precursors and porphyrins? c.) What is the safety and efficacy of currently used and new therapies for the porphyrias, especially in the long term?
Remember.Research is the Key to your cure!
Safe & Unsafe Drugs
Sunday - March 24, 2013 @ 19:45:35
Safe/Unsafe Drugs Dr. Peter V. Tishler, who is a porphyria expert at Harvard/ Brigham and Womens Hospital in Boston, has been instrumental in overseeing and updating the APF Safe/Unsafe Drug List for acute porphyria. Dr. Tishler is kindly updating the list again and wants your input. Therefore, if you have been negatively affected by a specific drug, please contact the APF. We will then put you directly in contact with Dr. Tishler to discuss your experience. When you report a drug, please have on hand, the name of the drug, the dose, and a synopsis of what happened to you when you took the drug. As you know, the Safe/Unsafe Drug List is extremely important for people with acute porphyrias, so your input is very important. It is often a lifesaving tool for the patients and their doctors. Dr. Tishler is a clinician/researcher in human genetics, including polycystic kidney disease, chronic obstructive pulmonary disease, Fabrys disease, and the porphyrias. We are fortunate to have porphyria specialists, like Dr. Tishler, to devote himself not only to our present health needs but to help assure a healthier future for each of us.
Remember.Research is the Key to your cure!
Porphyria Research is the Key to Your Cure
Friday - March 22, 2013 @ 22:35:32
Porphyria Research is the Key to Your Cure. Unfortunately, the numbers of patient volunteers is very small. More volunteers are needed. Please contact the APF if you are interested in participating in one or more of the research projects below directed by these experts: Karl Anderson, University of Texas Medical Branch, Galveston, TX; Dr. Robert Desnick, Mount Sinai School of Medicine, NYC, NY; Dr. Joseph Bloomer, University of Alabama, Birmingham, AL; Dr. Montgomery Bissell; University of California, San Francisco, CA; Dr. Herbert Bonkovsky, Carolinas Healthcare Systems, Charlotte, NC; and John Phillips, Ph.D. University of Utah, Salt Lake City, UT. â?¢ Mitoferrin-1 Expression in Patients with Erythropoietic Protoporphyria (EPP) â?¢ A double-blind, randomized, placebo-controlled, parallel group trial on the efficacy and safety of Panhematin in the treatment of acute attacks of porphyria â?¢ Clinical Diagnosis of Hereditary Coproporphyria (HCP) â?¢ Quantification of the Effects of Isoniazid Treatment on Erythrocyte and Plasma Protoporphyrin IX Concentration and Plasma Aminolevulinic Acid in Patients with Erythropoietic Protoporphyria â?¢ Hydroxychloroquine (HCQ) vs. Phlebotomy for Porphyria Cutanea Tarda â?¢ EPP: Natural History, Genotype-Phenotype Correlations, and Psychosocial Impact â?¢ A Pilot Study of Biomarkers Predicting Clinical Expression of Acute Porphyrias â?¢ Transplantation in EPP: A Review â?¢ Longitudinal Study of the Porphyrias National PORPHYRIA REGISTRY Only 650 people joined the Porphyria Registry. With so few people registering, the government funding agencies will NOT provide funding for porphyria research. They monitor if there are enough patients to warrant research funding. Porphyria experts created the Registry for you to share information about your health and as a means to learn from the experiences of many patients around the country. They will then use the knowledge to enhance diagnosis, treatment and find a cure for porphyria. Please take five minutes and sign up for the Porphyria Registry. Then you will be contacted by one of the research team. Joining the Porphyria Registry is anonymous and free, and all data is stored in a secure, computerized database. No personal identifying information will be given to anyone without your expressed approval. PLEASE TELL FAMILY MEMBERS WITH OR WITHOUT SYMPTOMS THAT THEY ARE NEEDED, TOO. Click on the Porphyria Registry button on the top line of the Home Page of the APF website, click on Join the Registry and locate the Porphyria Research Consortium and follow directions.
Remember.Research is the Key to your cure!
Spring Cleaning Naturally 101
Friday - March 22, 2013 @ 21:57:56
·
·
·
Clean Without Chemicals
Many people are conditioned to believe a house is not clean unless it smells of chemicals. In fact, the opposite is true. You can make your house sparkle with just a few simple supplies, many of which are already in your cupboards.
Mild Is Best
Mild dishwashing liquid is excellent for removing spills that water won't budge. Make a simple all-purpose cleaner by mixing 2 cups water with 2 tablespoons dishwashing liquid in a spray bottle. Use it on countertops and other hard surfaces.
Mild Is Best
Mild dishwashing liquid is excellent for removing spills that water won't budge. Make a simple all-purpose cleaner by mixing 2 cups water with 2 tablespoons dishwashing liquid in a spray bottle. Use it on countertops and other hard surfaces.
Natural Cleaners
Distilled white vinegar and lemon juice are both excellent for cleaning, deodorizing, and mild bleaching. They are acidic and can eliminate soap scum. Make a window- and mirror-cleaner by mixing equal parts vinegar and water, which also works well on most polyurethane-finished wood floors.
Less Is More
For routine cleaning, less is more. You actually need very few products to clean any given room. Although there will certainly be instances where specialized cleaners are necessary, the following list of products will suffice for most tasks. Gather them in a caddy so you can transport them from room to room as you work.
A Kit to Keep on Hand
Your universal cleaning kit should include:
·An all-purpose cleaner, or a solution of 2 tablespoons mild dishwashing liquid, such as Ivory, and 2 cups water in a spray bottle
·A mildly abrasive cleanser, such as Bon Ami
·A glass cleaner, or a solution of 1 part white vinegar and 1 part water in a spray bottle
·Rubber gloves; lint-free white cloths; medium-bristled scrub brush
Cleanliness isn't merely a virtue in the kitchen, the busiest room in your house: It is essential to the health and safety of your family. Corral your supplies in a bin or bucket stored in a cupboard under or near the sink. To protect the floor of the cupboard, line it with parchment paper or rubber matting.
Cleaning the Bathroom
Cleaning a bathroom well does not mean using harsh chemicals. Start with the gentlest cleaning solutions first before moving on to anything stronger. Adequate ventilation via a ceiling fan or open window will help prevent moisture buildup and go a long way toward keeping the bathroom fresh.
Remember.Research is the Key to your cure!
EPP & Rob Saupe
Tuesday - March 19, 2013 @ 11:07:46
Robert Saupè
Type of Porphyria:
Erythropoietic Protoporphyria (EPP)
When Robert was a baby, his mom went to hang up clothes outside and put him on the grass so she could watch him. After a short time, Robert started screaming and crying. For years, Robert was tested for various allergies, including grass pollen, soap and various foods. When Robert was nine years old, his mom took him to see a doctor who had just completed an internship under Dr. James Kushner, an expert in porphyrias. The doctor looked at Roberts hands and face, suspected that he had porphyria and told him to make an appointment with Dr. Kushner. Robert remembers going into the lab where Dr. Kushner did his testing. Dr. Kushner left the room, and when he came back he said, Bobby, you have porphyria. Dr. Kushner has called Robert Bobby ever since that day, and is the only person who calls him that. The nickname made Robert feel special. Dr. Kushner then kindly put a band-aid on Robert and wrote slugger on it, since Robert was starting baseball season. Everyone in Roberts family provided blood samples to trace the origin of his erythropoietic protoporphyria (EPP). Robert was tested every six months and at 16 he gave a core sample to be tested for research. Robert tried beta carotene, but the cost became prohibitive. Instead, he set out to build up a tan. He says that the more pigmentation he can get built into his skin, the better he can tolerate the sun. Unfortunately, building up the pigmentation can be terribly painful. Although Robert had his gallbladder removed as a result of a buildup of porphyrins, he does not let his EPP keep him from living his life. He goes fishing early in the morning and works outdoors. Due to his excavation job, Robert has had to manage his EPP very carefully. He protects himself everywhere he goes by wearing leather gloves, wide-brim hats, 100% cotton shirts and bandanas over his face. Robert works hard at photoprotection and copes with his EPP with humor. When a bystander saw Robert wearing a bandana at a NASCAR race, he asked if Robert had robbed a 7-11. Robert replied: shh, Im in hiding. Robert is very excited about participating in the Afamelanotide trials in Salt Lake City. He recently reconnected with his 22 year old twins, who live in Salt Lake City. Robert says that years ago he was a bad character, but he gave his life to the lord and completely changed. Robert now talks to his children every day and enjoys hearing his son say, Love you, Dad. Robert has been saving for his trip and is looking forward to seeing his children.
Attention ALL EPP Patients, Family & Friends
Tuesday - March 19, 2013 @ 10:58:27
EPP friends and family members please get your pen and paper out and write a letter to the FDA. The reason --- We need to assure them that people with EPP are in dire need of a treatment.
Many health professionals and health departments have the opinion that a life style change is all that is needed for people to handle EPP. In other words, some think that all you need to do is stay out of the sun, and you will be fine. People with EPP and their family members need to enlighten them that this is not true by presenting facts about your lives and the lives of your loved ones. We especially need to get this message across to FDA reviewers who will be assessing a new treatment, Afamelanotide / SCENESSE for approval.
Please take a few minutes of your time to write a letter to the FDA describing your experience with EPP, how it has negatively impacted your life and your family and how much you need a treatment for the disease. It would be helpful if those of you who were in the Phase II and Phase III trials and received the "real drug" share how the treatment changed your life in a positive way. Those who received the placebo can explain how much you desire effective treatment.
Your letters will accomplish far more than you can imagine. All you need to do is write the letter and address it to
Margaret Hamburg, M.D.
Commissioner, Food and Drug Administration
10903 New Hampshire Ave
Silver Spring, MD 20993-0002
*BUT DO NOT MAIL IT TO THEM*. Rather, send it to the APF, so that we can deliver all the letters to the FDA personally. We also ask if a few EPP patients who live in the DC area and are willing to speak with them in person would like to attend the meeting, as well. If you are willing to participate, please contact Desiree at the APF office 1.866.APF. 3635
This is a simple but important task that will only take you minutes. You have the opportunity to have a new treatment for EPP. Our researchers have worked very hard to complete the research for FDA approval. Please honor their work with your letter.
Remember. Research is the key to your cure!
Thank you,
Desiree Lyon Howe
Finding a Doctor
Tuesday - March 19, 2013 @ 11:01:33
Finding a Doctor
The American Porphyria Foundation promotes comprehensive care necessary for treating individuals with Porphyria. This section of our website offers suggestions for finding a local doctor who can manage your Porphyria, options for having your doctor consult a Porphyria specialist, and information on arranging a visit to a Porphyria clinic. Because Porphyria is so rare, few physicians have experience treating patients with the disease. Most patients are in fact treated But the APF can help by putting your doctor's office in touch with a Porphyria specialist who can offer guidance on your care. For those who need a diagnosis, you may be able to obtain a consultation at Porphyria clinic. Call the APF to reach a porphyria expert at a porphyria center. The APF office will also guide you to doctors who are not experts but are knowledgeable about porphyria. You may be asked to send your blood, urine, and stool samples for evaluation in advance of a clinic appointment. Especially if you plan to travel for a consultation, it is a good idea to call ahead and explain that you would like to be evaluated for Porphyria so that you can be sure you have done any necessary testing in advance. If local video conferencing facilities are available, telemedicine consultation with a Porphyria expert is also available. Regardless of your situation, it is best to establish a good relationship with a doctor in your area. Developing a relationship with a primary care physician takes time and can be frustrating, particularly when you have difficulty finding a doctor who will manage your care. In this section of the website, you will also find Tips for the Doctor's Office that may help. If you're having trouble finding a local doctor, the following organizations' doctor finder or physician referral services could be helpful. The APF does not recommend or endorse the doctors listed through these sites. American Medical Association American Society of Hematology American Association for the Study of Liver Diseases American Academy of Dermatology If you would like to read about supporting programs to ensure the quality of specialists in the field of porphyria, please see ourProtect Our Futurecampaign information.
Remember.Research is the Key to your cure!
Get Involved with the APF!
Tuesday - March 19, 2013 @ 10:51:00
Get Involved
Become a member of the American Porphyria Foundation today, and join us in our work for your good health!
When youjoin the APF, you become an integral part of an organization that empowers patients and helps them on the road to accurate diagnosis, proper care, and some day a cure. Adding your voice to ours makes us all stronger as we address our needs to health care providers, local, state and federal agencies and Congress.
Members of the American Porphyria Foundation receive:
Ourquarterly newsletter news about porphyria research and clinical studies, scientific meetings and member get-togethers, and stories about the doctors working in the porphyria field and about members like you;
Access to theAPF In Touch network the ability to connect with others who share your diagnosis;
Free participation in telephone conference calls with top researchers in the porphyria field;
Knowledgethat you are an important part of keeping reliable medical information about porphyria available to those who are newly diagnosed, or at a crossroads in their porphyria treatment, and frightened;
And much more!
The American Porphyria Foundation relies on member support to sustain programs like this website and other literature written or approved by porphyria experts.
U.S. memberships are $35 annually; international memberships are $45. The APF is a U.S. 501(c)(3) non-profit organization. All donations to the APF are tax deductible.
To join by phone with your VISA or MasterCard, call us toll-free at 1-866-APF-3635 Monday-Friday from 9:00 a.m. to 4:00 p.m. Central Time. To join by mail or fax, pleaseclick hereto complete and print the donation form.
Unable to pay? In case of need, we can waive the yearly $35/$45 membership donation. Simply write us a letter requesting that we waive the membership, sign and send it to the address below. We cannot accept waiver requests via email or telephone.
American Porphyria Foundation 4900 Woodway, Suite 780 Houston, TX 77056
Work with us!
The American Porphyria Foundation welcomes donations of your time and talents too. Would you like tovolunteerorraise money for the APF, organize or attend anevent, in addition to informing yourself about the porphyrias? If so, welcome! Youll find lots more information in this section of our website on opportunities to get involved in our, and you can always call our office for help: 1-713-266-9617. Ask for Mira.
The APF is here to serve, and were proud to have you with us.
Remember.Research is the Key to your cure!
A thought for the day
Monday - March 18, 2013 @ 16:08:06
Friends share & understand!
Did you know the people that are the strongest are usually the most sensitive? Did you know the people who exhibit the most kindness are the first to get mistreated? Did you know the one who takes care of others all the time are usually the ones who need it the most? Did you know the 3 hardest things to say are I love you, I'm sorry, and Help me. Sometimes just because aperson looks happy, you have to look past their smile and see how much pain they may be in. To all my friends who are going through some issues right now--Let's start an intention avalanche. We all need positive intentions right now. If I don't see your name, I'll understand. May I ask my friends wherever you might be, to kindly copy and paste this status for one hour to give a moment of support to all those who have family problems, health struggles, job issues, worries of any kind and just need to know that someone cares. Do it for all of us, for nobody is immune. I hope to see this on the walls of all my friends just for moral support. I know some will!! I did it for a friend and you can too. You have to copy & paste this one, no share button, because kindness is a effort given from the â?¥ not the press of a button.
I saw this on a FB site and it holds true for all. Enjoy & Share
Remember.Research is the Key to your cure!
From the Desk of Rob Saupe: EPP Patient
Monday - March 11, 2013 @ 13:20:56
From the Desk of Rob Saupe: EPP Patient
As many of you know I volunteered for another research opportunity with the Porphyria Consortium. I had the privilege of going to the Porphyria research lab at the University of Utah Medical Center and met with Dr. Parker and Dr. Phillips. The meeting went great and they are working very hard on different research projects for all the Porphyrias.
The Porphyria Consortium has been approved for a grant to help them continue doing research on the Porphyrias. The problem is that unless more people sign up they will not receive the funds necessary for all the research projects. Most of the research projects consist of you answering questions and maybe a blood draw. No Travel is necessary for the majority of the research studies. For the Blood draw they will send you a kit that includes a prepaid postage to ship it to the research lab. Just joining the registry so that there are more documented cases of Porphyria will help a lot! That simple!
Please, please join the registry today. And please consider joining one or as many of the research projects as you can. We have an opportunity to change our futures and the futures of our loved ones. It's now in our hands to make a difference. Be a solution and act today.
Click the link below and sign up. If you need help enrolling in the registry or help with logging into an existing account, please contact the APF office toll free at 1-866-APF-3635.
The Porphyria Research Consortium needs YOU. The Consortium can receive a government research grant as long as they have enough participants. At this point, they need 200 more patient volunteers.
Since the creation of the Research Consortium, they now have the best opportunity to make a major impact on the treatment of all of the porphyrias. But nothing can be accomplished without YOU.
I have had the privilege of participating in five research projects and hold a deep sense of personal gratification that patients around the country are now benefiting from that research. My family and I have volunteered for this newest research. I know that many of you would like to make this same sort of life saving contribution to people with porphyria.
At present, the researchers are performing a number of porphyria research projects. First, they have an ongoing Longitudinal Studythat requires that you answer a number of questions on a survey.
The researchers are also performing a very important research project with people who have an Acute Porphyria and have recurring attacks. If you have recurrent attacks or you are interested in volunteering for the equally important Longitudinal Study (for all Porphyrias), please contact the APF. After we share your name with the researchers, someone from the research team will contact you. Family members are also asked to participate in these research projects, as well.
In these studies, you are not required to take a new drug; rather, you are asked a series of questions. Please consider your participation in either or both projects. Nothing can be done to improve our treatment or diagnosis without our participation in the research project. Your time commitment will be very little compared to the great benefit for all.
For yours and your children's health, please consider volunteering as a research patient. Then call or email the APF with your contact information and the research team will shortly thereafter contact you.
This is your opportunity to be a part of life changing and lifesaving research.
Before Going to the Emergency Room consider these Tips. While having an Attack with Porphyria. Do you have a prepared bag to go at all times? Do you know what things to have with you and do you know what to say and when to ask questions. These are simple tools and tips that can help you have a better visit to the ER��
In 1996 over one half of the 90 million emergency room visits made in the US were considered unnecessary, pointing to a bizarre and costly trend among the Americanpublic to forego scheduling a doctors appointment in favor of simply going to the ER. This, despite the fact that routine emergency room costs are sometimes three times as much as a visit to a physicians office, a figure that does not include the time wasted waiting at the ERwhich, considering the system in place, is a substantial waste of time for non-urgent patients.
An Emergency room operates according to the triage system in an effort to make certain that the patients who need truly urgent care get that care. That system worksby instituting an evaluation system that, appropriately, moves certain patients to the front of the line. Those whose evaluation did not disclose an urgent case wait an average of around two hours before they are seen by a physician.
No one wants to wait two hours to be seen by a emergency room doctor when you do not feel well, especially in the lobby of a frantic emergency room. The following tips can prepare you for sudden medical problems and help you avoid spending so much wasted time at the emergency room.
The following tips are geared towards making certain you are prepared for a medical emergency so that you can make a more informed choice about whether or not to go to the ER.
Have a regular doctor
A regular physician, one with yourcompletemedical history and one who can arrange to see you in a moments notice, is your best defense against emergencies.
Research health care options in your area
Urgent care and minor emergency clinics are significantly cheaper than a visit to ahospitalER, they will most likely require less of your time, and you will still be seen by a licensed medical doctor.
Carry important medical information with you
Like themedical ID braceletsworn by people with food allergies or othermedical conditions, you should consider keeping, in your wallet or in yourpurse, important medical information about you as well, whether or not you have such a condition. The information should include:
â?¢ your doctors name and number â?¢ any illnesses you have â?¢ any medications you take and the dosage â?¢ whether or not you are pregnant
The information can prove valuable to any emergency medical care worker who is attempting to diagnose you.
Determine the kind of ERs at localhospitals Not all hospitals are equipped to handle every emergency. In fact, some hospitals don't have any emergency care. Emergency facilities are rated Level 1, 2 or 3. Those rated Level 3 are the most comprehensive trauma centers with high-tech equipment and specialists on the premises at all times. Level 1 and 2 centers can handle many kinds of emergencies, but may not have specialists on hand for some needs. Find out what type of emergency services are available at the medical facilities in your community.
Check with your insurance carrier
In short, not all emergencies are covered byhealth insurance. Those that are may have restrictions orinstructionsattached to them, such as the need to contact your carrier within a certain time frame after youve been admitted to the ER.
Call the ER before you leave
Calling ahead of time may reduce the time you wait at an ER, if it gives the staff a chance to get ready for your arrival. You will probably speak to a triage nurse, who may consider your symptoms overthe phonebut can not diagnose you. Depending on a number of factors, the nurse may or may not recommend that you:
â?¢ come in to the ER â?¢ call 911 and Emergency Medical Services â?¢ do or carry out certain things (such as stem any bleeding) before you reach thehospital â?¢ go to a different ER, one that is perhaps better equipped to deal with your emergency
A word toparents:Parentsought to give consideration to filing a consent form with your community ER that permits physicians to initiate medicaltreatmenton your child in the event you are unreachable for whatever reason. If a consent form like this makes you uncomfortable, bring up alternativeoptionswith your lawyer. Of course if you experience anysymptomsthat you believe to be an emergency, do not hesitateseek medical care immediately. Otherwise, be prudent about whether or not to seek the services of an emergency room.
If possible you might consider calling your regular doctor first and relaying to him or her what yoursymptomsare. The doctor can then advise you accordingly. Many physicians will work you into theirscheduleif they feel you need medical attention but do not need to visit an ER.
Primary care doctors are generally available 24 hours a day or they function within a group of doctors who rotate being on call at certain hours.
TheAmericanCollegeof Emergency Physicians (ACEP) recommends you familiarize yourself with the signs andsymptomsof illnesses and injuries such as those listed in the bookletHomeOrganizer for Medical Emergencies. For a complimentary copy, call ACEP at 800-446-9776.
Emergency Rooms: Considerations
Below are some guidelines and considerations you might give thought to when determining whether or not your condition warrants a visit to the ER.
Conditions that call for the ER
â?¢ Loss of consciousness â?¢ Signs of heart attack lasting longer than two minutes, such as: pressure, fullness, squeezing or pain in the center of the chest; tightness, burning, or aching under the breastbone; chest pain with lightheadedness; â?¢ Signs of a stroke, such as: sudden weakness or numbness of the face, arm or leg on one side of the body; sudden dimness or loss of vision, particularly in one eye; loss of speech, or trouble talking or understanding speech; sudden, severe headaches with no known cause; unexplained dizziness, unsteadiness or sudden falls, especially when accompanied by any other stroke symptom; â?¢ Significant shortness of breath; â?¢ Bleeding which, despite direct pressure for ten minutes, does not stop; â?¢ Instantaneous and severe pain; â?¢ Poisoning (Note: If at all possible, first contact the local poison control center; request immediately applicable advice, since some poisons must be vomited immediately and other poisons must be diluted withwaterimmediately. Actingquicklyin this manner can save a life.) â?¢ An allergic reaction to an insect bite, sting, ormedication, especially if breathing becomes labored (yoursymptoms will progressively get more severe) â?¢ Serious traumatic injury (i.e. to the head) â?¢ Unexplained stupor, drowsiness or disorientation. â?¢ Vomiting or coughing up blood. â?¢ Severe or persistent vomiting â?¢ Suicidal thoughts
Conditions that generally do not call for the ER
â?¢ Earaches; â?¢ Minorcutsin which bleeding has been stopped; â?¢ A bite from an animal which has stopped bleeding (nonetheless you should call your doctor in the event a rabies shot is required); â?¢ A broken bone (instead of the ER, contact your doctor. If that isnt possible, or if the fracture is evident, then head to the ER immediately). â?¢ A sprain, rash, sunburn or minor burn â?¢ Sting from an insect (unless you experience labored breathing; in that case, go to the ER or call 911 immediately). â?¢ Fever (if you are convulsive, then go to the ER). â?¢ Sexually-transmitteddiseases. (STDs) â?¢ Colds, coughs, a sore throat, orflu symptoms
"Remember. Research is the key to your cure!"
Low-energy bulbs 'worsen rashes from the BBC
Monday - March 4, 2013 @ 16:52:26
Low-energy bulbs 'worsen rashes'
Energy saving bulbs could reduce carbon dioxide emissions
The switch to energy-saving light bulbs may put thousands at risk of painful skin reactions, health charities warn.Fluorescent bulbs can exacerbate skin rashes in people with photosensitive skin conditions, experts said. The government is planning to prevent the sale of conventional bulbs by 2011 to cut carbon dioxide emissions. Several groups including the British Association of Dermatologists called for exemptions to allow those affected to continue using traditional bulbs. But representatives of the lighting industry said there would be alternatives to fluorescent lighting available. Health conditions which can involve some form of light sensitivity, include the auto-immune disease lupus, the genetic disorder Xeroderma Pigmentosum (XP), certain forms of eczema and dermatitis, photosensitivity, and porphyria.
We certainly don't want to say no to greener bulbs just that other bulbs need to be available
Andrew Langford, Skin Care Campaign
It has been estimated about 100,000 people in the UK with these skin conditions will be affected. Spectrum - an alliance of charities that support people with light sensitive conditions - says they have also been contacted with people suffering from ME who have had bad reactions to fluorescent light. Other groups have warned that low-energy bulbs, which use approximately a quarter of the energy of conventional bulbs, cause migraines and increase the risk of seizures in people with epilepsy. Phase-out Conventional or "incandescent" bulbs are being phased out in a voluntary agreement with retailers and will no longer be on sale from December 2011. Campaigners want people who have light sensitive conditions to be able to continue to buy conventional bulbs for their homes. They warned that employers must also be able to purchase incandescent lighting as employees have a right to such adjustments under the terms of the Disability Discrimination Act. Andrew Langford, chief executive officer of the Skin Care Campaign, one of the charities involved, said: "Incandescent light bulbs are the only source of electric light for many thousands of people with light sensitive conditions. "Add to this the thousands of people whose conditions or treatments may secondarily cause them to be light sensitive, and you have a large number of people potentially being isolated in the dark. "We certainly don't want to say no to greener bulbs just that other bulbs need to be available. "It's hard for people to understand what it's like to live with one of these conditions." He also called for a government-funded study into the effects of fluorescent lighting on photosensitive conditions as little research had been done to date. "We have the anecdotal information - it's a shame people don't listen to those affected. Dr Colin Holden, President of the British Association of Dermatologists, said: "It is important that patients with photosensitive skin eruptions are allowed to use lights that don't exacerbate their condition. "It is essential that such patients are able to protect themselves from specific wavelengths of light emitted by fluorescent bulbs, especially as they are often trapped indoors because they can't venture out in natural sunlight." Kevin Verdun, chief executive of the lighting association said only two-thirds of incandescent bulbs were being phased out. "These things have been taken into consideration and there will be bulbs they can still use. "There are also halogen bulbs and LED bulbs coming in in the next two or three years."
A service of the U.S. National Institutes of HealthHome is a great way to look of your type of Porphyria see what studies are under way and what studies have completed.
Just one more way to connect and help all Porphyria and rare Diseases!
The Porphyria Research Consortium needs YOU. The Consortium can receive a government research grant as long as they have enough participants. At this point, they need 200 more patient volunteers.
Since the creation of the Research Consortium, they now have the best opportunity to make a major impact on the treatment of all of the porphyrias. But nothing can be accomplished without YOU.
I have had the privilege of participating in five research projects and hold a deep sense of personal gratification that patients around the country are now benefiting from that research. My family and I have volunteered for this newest research. I know that many of you would like to make this same sort of life saving contribution to people with porphyria.
At present, the researchers are performing a number of porphyria research projects. First, they have an ongoing Longitudinal Study that requires that you answer a number of questions on a survey.
The researchers are also performing a very important research project with people who have an Acute Porphyria and have recurring attacks. If you have recurrent attacks or you are interested in volunteering for the equally important Longitudinal Study (for all Porphyrias), please contact the APF. After we share your name with the researchers, someone from the research team will contact you. Family members are also asked to participate in these research projects, as well.
In these studies, you are not required to take a new drug; rather, you are asked a series of questions. Please consider your participation in either or both projects. Nothing can be done to improve our treatment or diagnosis without our participation in the research project. Your time commitment will be very little compared to the great benefit for all.
For yours and your children's health, please consider volunteering as a research patient. Then call or email the APF with your contact information and the research team will shortly thereafter contact you.
This is your opportunity to be a part of life changing and lifesaving research.
Introducing as guest Role the American Porphyria Foundation & You Tube Channel have joined together to create some exciting videos for you to watch. These videos are approved by the APF. The videos discuss Informative Information like the importance about DNA testing and research. Take a look into the APF, Patient Stories, and a step by step instruction video on how to administer the Drug Panhematin. A wonderful explanation about Porphyria from Porphyria experts Dr. Karl Anderson and many others. Be sure to subscribe today to stay up on the latest Videos and News. Please feel free to encourage family, friends and medical personnel to understand more about the Porphyrias.
What is Rare Connect? Once you sign up it's free and you become a member. You are Connecting with Patients of Rare disease Globally! There is Information from many of the Porphyria Centers worldwide, we ask questions, we talk, we read and join in excellent conversations! So if you see any familiar faces say "HI" and become friends and if you or know someone with another disease join that group to. We are excited for all of you to join in this process. All groups are monitored and all have good guidelines to follow and it's so simple to use. If you have any problems or signing up please contact AmyLChapman1992@gmail.com and she will be happy to assist you.
Find an online community for your area of interest. Meet, interact and learn from your peers and medical experts. We have 39 rare disease communities with more to come soon!
Meet and interact with others who share your condition in a supportive and friendly environment. Find the information and support you need and share your own experiences.
Vittoria's Story - Hello my friends, my name is Vittoria and I am very happy to make your Read more >
Events
4th International WM Patient Forum - WMUK will be one More >
Wochenendseminar für Betroffene und Familien mit Tyr More >
2nd Meeting of VHL Patient Group Leaders - For furthe More >
- See more at: https://www.rareconnect.org/en#sthash.8Z3sQ5Sk.dpuf
Rare Disease Day February 28th 2013
Wednesday - February 20, 2013 @ 20:24:01
Rare Disease Day
February 28th 2013
Rare Disease Day is an international advocacy day to bring widespread recognition of rare diseases as a global health challenge. The day is celebrated on the last day of February every year. In 2013, it will be observed on February 28th.
Anyone can be involved in Rare Disease Day. The day has been established as a grassroots advocacy day and we encourage everyone to participate in some way!
What is a Rare Disease?
In the U.S., any disease affecting fewer than 200,000 people is considered rare. This definition comes from the Orphan Drug Act of 1983 and is slightly different from the definition used in Europe. There are nearly 7,000 rare diseases affecting nearly 30 million Americans. In other words, almost one in ten Americans are suffering from rare diseases.
Besides dealing with their specific medical problems, people with rare diseases struggle to get a proper diagnosis, find information, and get treatment. The rarity of their conditions makes medical research more difficult.
Working together across the World we all can make a difference. Please get involved in every opportunity to bring awareness to Porphyria and the many other rare diseases that affect so many people.
Remember..Research is the key to your cure!
Why Is Getting A Rare Disease Diagnosis So Difficult?
Tuesday - February 19, 2013 @ 17:28:34
Why Is Getting A Rare Disease Diagnosis So Difficult?
It can be a long, frustrating process
·From:NIH
Getting a rare disease diagnosis can be a long, frustrating process
Getting a correct diagnosis is often a major challenge for someone who has a rare disease. Many people are unable to get a diagnosis, are misdiagnosed or have one diagnosis then another. There are many reasons why getting a rare disease diagnosis can be a long, frustrating experience.
Your disease is rare
It may seem obvious, but the very fact that a disease is rare makes it very difficult to be recognized. You may see many doctors before you finally find one who knows something about what you have. Some diseases are so rare that only a geneticist (genetics specialist) would be able to identify them aftergenetic testingis done.
Some rare diseases have symptoms, such as weakness, anemia, pain, vision problems, dizziness or coughing. Many different diseases can cause these symptoms, so they are called nonspecific, meaning they are not signs of a specific disease. Doctors are trained to look at more common causes of symptoms first, so they may not be thinking along the lines of a rare disease when they examine you.
Your symptoms are unusual
It seems logical that having an unusual symptom would help in pinpointing a diagnosis. This is true if the doctor examining you is familiar with a disease that causes the symptom. If he or she doesnt know of any disease that causes the symptom, then most likely you will be referred to a specialist who may know something about your condition.
You dont have 'textbook' symptoms
You may have a rare disease, but your symptoms do not fit the classic or typical picture of the disease. You may have symptoms that dont usually go along with the disease, or you may not have all the symptoms that are expected with the disease. Doctors may hesitate to diagnose you with the rare disease because of this.
You have been waiting forever to see a specialist
Its difficult to get an appointment with some doctors, most of all those who specialize in rare diseases. It may be 3 to 6 months before you can see someone who has a heavy schedule. It can be disappointing to wait a long time only to be told that theyre not sure what you have or that they want you to go see another specialist.
I know a mother of a child with a rare disease who has typed up some pages explaining what her daughters disease is, her medical and surgical history and her current medications. The mother hands copies of these pages to each new doctor who examines her daughter so she wont have to repeat everything yet again. You may feel as frustrated as she does, having to give the same information many times. It may seem as if the doctors dont read your chart or look at your test results. Seeing new doctors adds to the stress of getting a diagnosis.
Sometimes, despite seeing the best specialists, you cant get a correct diagnosis. Doctors may use words such as of unknown etiology or idiopathic (meaning, we dont know what causes it) or atypical (meaning unusual). You may be given a diagnosis that best fits your symptoms, or given two or more diagnoses together.
Recognizing that people with rare diseases may have difficulty getting a diagnosis, the U.S. National Institutes of Health (NIH) started theUndiagnosed Diseases Programin September 2008. This research program will evaluate 50 to 100 cases of undiagnosed diseases to try to provide answers to people with mysterious conditions and to advance medical knowledge about the diseases. If you have a medical condition but no diagnosis, talk with your doctor about participating in this program. Information specialists at the Clinical Centers Recruitment Call Center (1-866-444-8806) can provide more information about eligibility and what kinds of medical information your doctor needs to submit for review.
Protect our future
Monday - February 11, 2013 @ 16:35:14
Protect our future
The Protect Our Future campaign was established to attract and train the next generation of doctors and specialists in the field of Porphyria. Over the next decade, we will lose ninety percent of our valued Porphyria experts. These men and women have led Porphyria research, testing and treatment for the past 30 years. Without financial support, we run the risk of losing knowledge of the disease, quality testing, diagnosis, and treatment, and ultimately a cure.
When we originally made the Protect Our Future appeal, the APF received a higher volume of payments for annual memberships. We appreciate your contributions, which help fund patient and physician educational programs.
Protect Our Future is a separate campaign and need. We are seeking additional donations for the specific purpose of locating and training new porphyria specialists.
You and I are pulled in so many directions for our donations, such as churches, police leagues and schools. But rarely will we be presented with an opportunity to affect the course of our own lives and those of our children for years to come.
Please consider a donation or fundraiser to support this goal.
Lets work together to bring another great specialist into our lives. We are so very fortunate to have the few porphyria experts who are presently in the field. Now we can protect our own future by adding more doctors.
Donate now! Please make a note that you are donating to the Protect Our Future campaign so that we can allocate those funds appropriately.
Getting an accurate diagnosis was a long and complicated journey for Amy. For two decades she coped with debilitating symptoms while her doctors worked to identify the source of her pain. Watch this video to learn how Amy educated herself and worked with her doctors to finally get diagnosed with AIP.
Would you like to Tell your story about Porphyria?
Sunday - February 10, 2013 @ 17:00:35
HI there all! I hope that everyone is doing well at this time. I am looking for those who might be willing to share there story about Porphyria and what struggles they have and how they have been able to get back to better health. We all need help and ideas so please take a moment to think about this invite and if you would like to share your thoughts and stories please email me @ AmyLChapman1992@gmail.com
Self-esteem: 4 steps to feel better about yourself!
Friday - February 1, 2013 @ 04:12:05
Self-esteem: 4 steps to feel better about yourself
I know that having Porphyria can be very difficult at times but when I read this over it really made me think about how I view things and how I can change them. Once you put them into practice I know you will feel better about yourself but your life to. Enjoy:)
If you have low self-esteem, harness the power of your own thoughts and beliefs to change how you feel about yourself. Start with these four steps to a healthier self-esteem.
Low self-esteem can negatively affect virtually every facet of your life, including your relationships, your job and your health. But you can take steps to boost your self-esteem, even if you've been harboring a poor opinion of yourself since childhood. Start with these four steps.
Step 1: Identify troubling conditions or situations
Think about the conditions or situations that seem to deflate your self-esteem. Common triggers might include:
·A business presentation
·A crisis at work or home
·A challenge with a spouse, loved one, co-worker or other close contact
·A change in life circumstances, such as a job loss or a child leaving home
Step 2: Become aware of thoughts and beliefs
Once you've identified troubling conditions or situations, pay attention to your thoughts about them. This includes your self-talk what you tell yourself and your interpretation of what the situation means. Your thoughts and beliefs might be positive, negative or neutral. They might be rational, based on reason or facts, or irrational, based on false ideas.
Step 3: Challenge negative or inaccurate thinking
Your initial thoughts might not be the only possible way to view a situation so test the accuracy of your thoughts. Ask yourself whether your view is consistent with facts and logic or whether other explanations for the situation might be plausible.
Be aware that it's sometimes tough to recognize inaccuracies in thinking, though. Most people have automatic, long-standing ways of thinking about their lives and themselves. These long-held thoughts and beliefs can feel normal and factual, but many are actually just opinions or perceptions.
Also pay attention to thought patterns that tend to erode self-esteem:
·All-or-nothing thinking. You see things as either all good or all bad. For example, "If I don't succeed in this task, I'm a total failure."
·Mental filtering. You see only negatives and dwell on them, distorting your view of a person or situation. For example, "I made a mistake on that report and now everyone will realize I'm not up to this job."
·Converting positives into negatives. You reject your achievements and other positive experiences by insisting that they don't count. For example, "I only did well on that test because it was so easy."
·Jumping to negative conclusions. You reach a negative conclusion when little or no evidence supports it. For example, "My friend hasn't replied to my email, so I must have done something to make her angry."
·Mistaking feelings for facts. You confuse feelings or beliefs with facts. For example, "I feel like a failure, so I must be a failure."
·Self put-downs. You undervalue yourself, put yourself down or use self-deprecating humor. This can result from overreacting to a situation, such as making a mistake. For example, "I don't deserve anything better."
Step 4: Adjust your thoughts and beliefs
Now replace negative or inaccurate thoughts with accurate, constructive thoughts. Try these strategies:
·Use hopeful statements. Treat yourself with kindness and encouragement. Pessimism can be a self-fulfilling prophecy. For example, if you think your presentation isn't going to go well, you might indeed stumble through it. Try telling yourself things such as, "Even though it's tough, I can handle this situation."
·Forgive yourself. Everyone makes mistakes and mistakes aren't permanent reflections on you as a person. They're isolated moments in time. Tell yourself, "I made a mistake, but that doesn't make me a bad person."
·Avoid 'should' and 'must' statements. If you find that your thoughts are full of these words, you might be putting unreasonable demands on yourself or on others. Removing these words from your thoughts can lead to more realistic expectations.
·Focus on the positive. Think about the good parts of your life. Remind yourself of things that have gone well recently. Consider the skills you've used to cope with challenging situations.
·Relabel upsetting thoughts. You don't need to react negatively to negative thoughts. Instead, think of negative thoughts as signals to try new, healthy patterns. Ask yourself, "What can I think and do to make this less stressful?"
·Encourage yourself. Give yourself credit for making positive changes. For example, "My presentation might not have been perfect, but my colleagues asked questions and remained engaged which means that I accomplished my goal."
These steps might seem awkward at first, but they'll get easier with practice. As you begin to recognize the thoughts and beliefs that are contributing to your low self-esteem, you can actively counter them which will help you accept your value as a person. As your self-esteem increases, your confidence and sense of well-being are likely to soar.
International Meeting of Porphyria Patients
Friday - February 1, 2013 @ 04:24:16
International Meeting of Porphyria Patients
The International Porphyria Patient Day, organized by the Swiss Society for Porphyria and the German EPP Patient Group, will be held on Saturday, May 18th, 2013 in Lucerne, Switzerland.
The primary objectives of the Patient Day:
networking between individual patients, their organizations and the scientific experts in the field of porphyria
sharing information on the latest research activities and clinical advances
discussing international collaborations between patient organizations and planning for an international umbrella organization to more effectively protect patients' well-being and promote their interests
The Swiss Society for Porphyria and the German EPP Patient Group would like to encourage representatives from the various international patient associations and individual porphyria patients to attend the Patient Day.We hope to see many of you there: numerous participants will contribute to making this day an enriching and valuable event for the cause of porphyria patients around the world.
Some scholarship funding will be available, so if you are interested in attending and /or needing a small scholarship, please contact the APF toll free: 1.866.APF.3635
This will be a rare opportunity to bring together Canadians withporphyria, their family members, medical professionals and researchers. Please join them at this exciting conference!
The Alberta Porphyria Society afternoon break out session will include a presentation by Dr. Brian Gilfix of McGill University, Montreal, Quebec. Dr. Gilfix had served on the Advisory Board of the Canadian Association for Porphyria. You can read his article, Lab Investigation of the Porphyrias on the Alberta Porphyria Society website.
Remember..Research is the key to your cure!
National Porphyria Awareness Week April 14-20, 2013 is about YOU!
Tuesday - January 15, 2013 @ 16:16:52
National Porphyria Awareness Week April 14-20, 2013 is about YOU!
The challenge of living with porphyria starts with how little is known about it among friends, family and the medical community. You are the way this group of people can be reached. During National Porphyria Aware-ness Week April 14-20, 2013 (NPAW), YOU have the opportunity to enhance porphyria awareness in your sphere of influence. Here are some suggestions for ways that you can help: *SHARE knowledge about porphyria at your doctors offices and local hospitals. You might suggest that they host a seminar or grand rounds on porphyria; ask if there is a local meeting where you can hand out materials. *ASSIST at medical conventions or health fairs to educate laypersons and physicians on porphyria. *TELL your story to local media. Television, newspapers, community magazines are looking for human interest stories about people who have encountered a major illness and have undertaken the challenge. *VOLUNTEER your talents or skills to help achieve the educational programs of the APF. For example, donate one of your paintings, sculpture, computer expertise, business acumen etc. for our fall raffle or to help APF. *HOLD a community race, car wash or other fund raising activity. *HONOR your loved one with a gift to the APF for a birthday, anniversary, holiday or memorial tribute. *WRITE a letter to friends and family asking them to consider making a donation to the APF; *ASK your local newspaper or community newsletter to include a story about you and porphyria or just do an article on porphyria. Every article helps increase awareness. *LEARN how to be an advocate in your daily life. There are many opportunities to share knowledge of porphyria. *BEFRIEND your physicians and they will share their new found knowledge of the disease. *HOST a patient meeting and share your experiences and your successes in advancing porphyria awareness. The APF can help you accomplish these goals by providing materials: Porphyria Brochures, A Porphyria Live DVD, Fact sheets, Powerpoint Presentations, Information for Grand Rounds, Ideas to set up Medical Seminars and Health Fairs, Information to gain press coverage, Press Releases for local newspapers and television and many more.
As 2013 begins, surround yourself with the things in your life that make you happy: friends, family, pets. Think about what you are grateful to have, rather than what you dont have. Also, be sure to show gratitude to others; has your staff been working overtime? Studies show that showing gratitude to your employees can improve work performance.
Take Time for Yourself
Dont let your hectic schedule get in the way of taking a little time for you. Take a break. What about getting your nails done, a nice dinner with someone special, read a good book or even taking a good nap. What would you do with some more you time? Spend time with your kids, maybe volunteering?
Turn off the TV
A study from the University of Maryland correlates TV watching with lower levels of happiness. So turn off the tube and get out there! Take a walk in the park, read a book or try something new. If you watched one less hour of TV a day, what could you accomplish?
Be a Do-Gooder
And bring out the good in other people by helping out! The benefits of volunteering are endless: Make friends, learn new skills, expand your resume, teach values to your kids, strengthen your sense of communityâ?¦ What else? Tell us in the comments!
Meet other do-gooders. Meeting new friends while volunteering can expand your social or professional network. What a great way to join the APF FB groups and share your stories and experience. And of course, its fun!
Dont wait for the right moment
Theres no time like the present to jump in and volunteer. Your local nonprofits always need your help! Find a charity near you.
Donate What you Can
Studies show that giving to others makes us happy. Cant make the financial commitment? Give your time or expertise. How can you support the APF as an individual or a family? Or donate goods that you no longer use: clothes, food, school supplies, etc.
Want to learn a new skill, or teach your kids one, but dont know where to start? Browse opportunities with local arts nonprofits. Need career help? Browse job training nonprofits near you. Remember Research is the Key!
TV, Books, Shows on Porphyria Watch & Read!
Friday - January 4, 2013 @ 17:27:08
TV, Books, Shows on Porphyria
From: Desiree Lyon~We were asked to repost the many tv shows that the apf was able to convince the networks to do on porphyria. Except the bad csi one. Here goes a few are missing *House, Honeymoon, Season 1: episode 22*House, Fools for Love, Season 3: episode 5 (mentions porphyria)*House, Finding Judas, Season 3: episode 9*House, Dont ever Change, Season 4: episode 12 (mentions porphyria)*House, Guardian Angels, Season 4: episode 4 (mentions porphyria)*House, Whatever it takes, Season 4: episode 6 (mentions porphyria)*House, Itch, Season 5: Episode 7*House, Emancipation, Season 5: episode 8 (mentions porphyria)*House, Let them eat cake, Season 5: Episode 10*House, Carrot or Stick , Season 7, Episode 10
*Scrubs, My Ocardial Infarction: Season 4, Episode 13*Scrubs, Kelsos last stand,Season7: episode 9*Scrubs, My Dumb Luck, Season 9: episode 7*Scrubs: Outta here like Vladimir: Season 8, Episode 4
*Grays Anatomy, Time Warp Season 6 episode 15
*Castle, Vampire Weekend, Season 2 , Episode 6
*Doc Martin, Series 4, Episode 2*CSI Las Vegas, Justice Served Season 1 Episode 21*CSI Las Angeles, Once Bitten , Twice Damned Season 2 Episode ?
*ABC News Specials, Medical Mysteries Series, episode 2**ABC News Desiree Lyon interview *ABC Prime Time CEP segment
*Mystery Diagnosis, The Sickest Patient in the Hospital and Terrifying Tremors, Season 5*Mystery Diagnosis, The Boy Who Kept Swelling, Season 6 episode 6
*Mystery ER, Seeping through the cracks/Purple Haze, Season 1: episode 3
*Secret History: Purple Secret in Search of Royal Madness, Season 6: episode 6
*Montel Williams: Porphyria with Lauren Warren*Montel Williams, Rare Diseases, Leppert Family
*Travel Channel, Documentary Romania
*Learning Channel Dec 09 Porphyria, another myth in the making.
*Fox News Desiree Lyon interview*Fox News Vampires , A Medical Myth Nov 2009*Fox News King George, Madness or Arsenic July 2005
*National Geographic; Feb 2010 Six Ways to Stop A Vampire
*Court TV
_________________________________________________________________________________Parade Magazine, Desiree Lyon Howe stroyParade Magazine, Porphyria, Rare Disease FeatureNew York Time Magazine-Sunday, Perplexing Pain : Porphria Article_________________________________________________________________________________*The Madness of King George (1994) & (2005) Movie
NBC Evening News , Thurs. May 31 185Dr. Bruce Spielgaman WBZ Aug 25 2005Jenkins, Mark Collins. Vampire forensics: Uncovering the origins of an enduring legend. Washington: National Geographic, 2010. 303pp. Porphyria Featured on Television
*House, Honeymoon, Season 1: episode 22*House, Fools for Love, Season 3: episode 5 (mentions porphyria)*House, Finding Judas, Season 3: episode 9*House, Dont ever Change, Season 4: episode 12 (mentions porphyria)*House, Guardian Angels, Season 4: episode 4 (mentions porphyria)*House, Whatever it takes, Season 4: episode 6 (mentions porphyria)*House, Itch, Season 5: Episode 7
*House, Let them eat cake, Season 5: Episode 10*House, Carrot or Stick , Season 7, Episot 10
*Scrubs, My Ocardial Infarction: Season 4, Episode 13*Scrubs, Kelsos last stand,Season7: episode 9*Scrubs, My Dumb Luck, Season 9: episode 7*Scrubs: Outta here like Vladimir: Season 8, Episode 4
*Grays Anatomy, Time Warp Season 6 episode 15
*Castle, Vampire Weekend, Season 2 , Episode 6
*Doc Martin, Series 4, Episode 2*CSI Las Vegas, Justice Served Season 1 Episode 21*CSI Las Angeles, Once Bitten , Twice Damned Season 2 Episode ?
*ABC News Specials, Medical Mysteries Series, episode 2**ABC News Desiree Lyon interview *ABC Prime Time CEP segment
*Mystery Diagnosis, The Sickest Patient in the Hospital and Terrifying Tremors, Season 5*Mystery Diagnosis, The Boy Who Kept Swelling, Season 6 episode 6
*Mystery ER, Seeping through the cracks/Purple Haze, Season 1: episode 3
*Secret History: Purple Secret in Search of Royal Madness, Season 6: episode 6
*Montel Williams: Porphyria with Lauren Warren*Montel Williams, Rare Diseases, Leppert Family
*Travel Channel, Documentary Romania
*Learning Channel Dec 09 Porphyria, another myth in the making.
*Fox News Desiree Lyon interview*Fox News Vampires , A Medical Myth Nov 2009*Fox News King George, Madness or Arsenic July 2005
*National Geographic; Feb 2010 Six Ways to Stop A Vampire
*Court TV
*Midsommer Murders: Season 13, Episode 5 Masterclass_________________________________________________________________________________Parade Magazine, Desiree Lyon Howe stroyParade Magazine, Porphyria, Rare Disease FeatureNew York Time Magazine-Sunday, Perplexing Pain : Porphria Article_________________________________________________________________________________*The Madness of King George (1994) & (2005) Movie
NBC Evening News , Thurs. May 31 185Dr. Bruce Spielgaman WBZ Aug 25 2005Jenkins, Mark Collins. Vampire forensics: Uncovering the origins of an enduring legend. Washington: National Geographic, 2010. 303pp.
Thought for the day.
Friday - January 4, 2013 @ 21:40:50
A good reminder to one's self. If you agree with this statement please hit like or agree or feel free to share your thoughts!
























.JPG)































 For therapy, a caring doctor had recommended I write about my illness, that I state what it has done to me and how it has affected my life and finally, what I hope will happen no matter how unrealistic. Since it took a better part of my lifetime to unravel the mysterious maladies that plagued me most of my life, it was difficult to write about it in a less compassionate form. It is important to understand when you read this that it is possible to have been born with more than one congenital anomaly. In my case, I was born with a mild Arnold Chiari Malformation which accounts for an inability to nurse, dizziness and clumsiness in infancy and adolescence. Porphyria symptoms were not present until my early to mid-teens.
For therapy, a caring doctor had recommended I write about my illness, that I state what it has done to me and how it has affected my life and finally, what I hope will happen no matter how unrealistic. Since it took a better part of my lifetime to unravel the mysterious maladies that plagued me most of my life, it was difficult to write about it in a less compassionate form. It is important to understand when you read this that it is possible to have been born with more than one congenital anomaly. In my case, I was born with a mild Arnold Chiari Malformation which accounts for an inability to nurse, dizziness and clumsiness in infancy and adolescence. Porphyria symptoms were not present until my early to mid-teens.


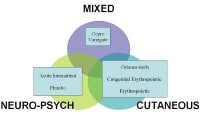


 Tom Collier and his brother both suffered the symptoms of Erythropoietic Protoporphyria nearly all their lives, but until recently they had no explanation for their photosensitivity. Diagnosis finally came when Tom was 64 years old, after a lifetime searching for answers.
Tom Collier and his brother both suffered the symptoms of Erythropoietic Protoporphyria nearly all their lives, but until recently they had no explanation for their photosensitivity. Diagnosis finally came when Tom was 64 years old, after a lifetime searching for answers. Purple.jpg)














.jpg)

















 Cathleen Mouledoux does not have EPP, but she knows the disease well because her daughter Celeste suffers from it. The disease is in Cathleens husbands family, but Rene was never troubled by it, playing outside all the time as a child without anything more than a sunburn. Rene was only tested for Erythropoietic Protoporphyria until after he and Cathleen found out their little girl had EPP.
Cathleen Mouledoux does not have EPP, but she knows the disease well because her daughter Celeste suffers from it. The disease is in Cathleens husbands family, but Rene was never troubled by it, playing outside all the time as a child without anything more than a sunburn. Rene was only tested for Erythropoietic Protoporphyria until after he and Cathleen found out their little girl had EPP. As a toddler Celeste had a bad burning sensation in the skin on her hands when she was exposed to the sun. Nothing Cathleen tried eased the pain, but there were no visible symptoms. Then when Celeste was about four years old, she broke out in tiny little bumps that looked like bug bites after being out in the sun. The family called them spider eyeballs and again Celeste suffered terrible pain with sun exposure.
As a toddler Celeste had a bad burning sensation in the skin on her hands when she was exposed to the sun. Nothing Cathleen tried eased the pain, but there were no visible symptoms. Then when Celeste was about four years old, she broke out in tiny little bumps that looked like bug bites after being out in the sun. The family called them spider eyeballs and again Celeste suffered terrible pain with sun exposure.



 APF Sponsor, Jennie Eberhardt, has been awarded the 2006 APF Ambassador for the work she has done in her community. She is a one-woman porphyria awareness dynamo. Before her illness, Jennie enjoyed a successful career as a professional make-up artist with theaters and photographers. Her work took on other unusual aspects. For instance, she created mock victims to help train ambulance crews for disaster drills. She also did the make-up for cancer patients. One of her most gratifying experiences was to create a jaw line for a woman who had lost part of her jaw to throat cancer surgery. But her most enjoyable career experience was as the make-up artist for a production with female impersonators. In fact, Jennie developed such a great relationship with her clients that they are now some of her biggest supporters and encouragers since her illness.
APF Sponsor, Jennie Eberhardt, has been awarded the 2006 APF Ambassador for the work she has done in her community. She is a one-woman porphyria awareness dynamo. Before her illness, Jennie enjoyed a successful career as a professional make-up artist with theaters and photographers. Her work took on other unusual aspects. For instance, she created mock victims to help train ambulance crews for disaster drills. She also did the make-up for cancer patients. One of her most gratifying experiences was to create a jaw line for a woman who had lost part of her jaw to throat cancer surgery. But her most enjoyable career experience was as the make-up artist for a production with female impersonators. In fact, Jennie developed such a great relationship with her clients that they are now some of her biggest supporters and encouragers since her illness.












 Many of the counselors have skin conditions as well, and can provide support and advice to campers. Fun, friendship, and independence are on the top of everyones agenda and everyone shares in the discovery of what its like to be included.
Many of the counselors have skin conditions as well, and can provide support and advice to campers. Fun, friendship, and independence are on the top of everyones agenda and everyone shares in the discovery of what its like to be included.




 My name is Charles Preuss Johnson and I have Acute Intermittent Porphyria (AIP). I was named after my maternal grandfather, Charles Preuss, who came to the U.S. from Germany and who died at age 39 after several bouts of severe abdominal pain. They removed his appendix, and he still had acute pain. His daughter, my mother Lorraine Preuss, died at age 49 after nine weeks hospitalized from symptoms of AIP. She suffered her whole life never knowing that her acute abdominal pain had a diagnosis of porphyria. She was a mere 67 pounds when she was finally diagnosed and that was only a few days before she died.
My name is Charles Preuss Johnson and I have Acute Intermittent Porphyria (AIP). I was named after my maternal grandfather, Charles Preuss, who came to the U.S. from Germany and who died at age 39 after several bouts of severe abdominal pain. They removed his appendix, and he still had acute pain. His daughter, my mother Lorraine Preuss, died at age 49 after nine weeks hospitalized from symptoms of AIP. She suffered her whole life never knowing that her acute abdominal pain had a diagnosis of porphyria. She was a mere 67 pounds when she was finally diagnosed and that was only a few days before she died. My daughter Rebekah has Erythropoietic Protoporphyria. We live in the Grand Rapids, MI area.
My daughter Rebekah has Erythropoietic Protoporphyria. We live in the Grand Rapids, MI area.




 I spent my whole life with unexplained symptoms. Sometimes my legs would give out, and I would have back pain, abdominal pain, slurred speech, difficulties walking and so forth. When I was 16, doctors found a mass in my brain. After removing what they could, all my health problems were blamed on post surgical changes.
I spent my whole life with unexplained symptoms. Sometimes my legs would give out, and I would have back pain, abdominal pain, slurred speech, difficulties walking and so forth. When I was 16, doctors found a mass in my brain. After removing what they could, all my health problems were blamed on post surgical changes.
 It's hard to believe it's been thirty years since my diagnosis. I thought life as I had known it was over. I had a loving husband, two wonderful children and nothing really bad had ever happened to me. I found out at the age of thirty that I was going to have another child. Everything went fairly well up until about five months into the pregnancy. I began to have abdominal pains. The pain would come and go. I would go into the hospital, stay a while, be diagnosed with false labor and given medication. In and out- In and out. The pain, however, became increasingly worse and was accompanied by nausea and vomiting. I also had a strange thing start happening. My urine turned tea colored.
It's hard to believe it's been thirty years since my diagnosis. I thought life as I had known it was over. I had a loving husband, two wonderful children and nothing really bad had ever happened to me. I found out at the age of thirty that I was going to have another child. Everything went fairly well up until about five months into the pregnancy. I began to have abdominal pains. The pain would come and go. I would go into the hospital, stay a while, be diagnosed with false labor and given medication. In and out- In and out. The pain, however, became increasingly worse and was accompanied by nausea and vomiting. I also had a strange thing start happening. My urine turned tea colored.












 I was diagnosed with Porphyria Cutantea Tarda (PCT) in 1983 at age thirty seven. I had always had horrendous skin and infections of the skin. Within twenty-four hours of sunbathing, I broke out in patches of blisters on my forearms. This was the first symptom. But for a long time before this, my hair had been growing much faster than normal and my fingernails would split and crack off the top layer. My face had developed a brown racoon mask. But I didn't feel ill.
I was diagnosed with Porphyria Cutantea Tarda (PCT) in 1983 at age thirty seven. I had always had horrendous skin and infections of the skin. Within twenty-four hours of sunbathing, I broke out in patches of blisters on my forearms. This was the first symptom. But for a long time before this, my hair had been growing much faster than normal and my fingernails would split and crack off the top layer. My face had developed a brown racoon mask. But I didn't feel ill.










































 Meghann Bauer has had symptoms of erythropoietic protoporphyria (EPP) since she was a little baby, yet her parents took her to different doctors for years before she was diagnosed at age 16 with EPP.
Meghann Bauer has had symptoms of erythropoietic protoporphyria (EPP) since she was a little baby, yet her parents took her to different doctors for years before she was diagnosed at age 16 with EPP.















 When Robert was a baby, his mom went to hang up clothes outside and put him on the grass so she could watch him. After a short time, Robert started screaming and crying. For years, Robert was tested for various allergies, including grass pollen, soap and various foods. When Robert was nine years old, his mom took him to see a doctor who had just completed an internship under Dr. James Kushner, an expert in porphyrias. The doctor looked at Roberts hands and face, suspected that he had porphyria and told him to make an appointment with Dr. Kushner.
When Robert was a baby, his mom went to hang up clothes outside and put him on the grass so she could watch him. After a short time, Robert started screaming and crying. For years, Robert was tested for various allergies, including grass pollen, soap and various foods. When Robert was nine years old, his mom took him to see a doctor who had just completed an internship under Dr. James Kushner, an expert in porphyrias. The doctor looked at Roberts hands and face, suspected that he had porphyria and told him to make an appointment with Dr. Kushner.











